






1. Introduction
Empathy (also called sympathy or transference) is regarded by psychologists both in China and abroad as a key trait in high-level psychological counseling and psychotherapy relationships. It is not merely about feeling the problem from the other person’s perspective, but also about transcending the problem to discover the meaning of solving it and making one’s own judgments and providing help [1]. When nurses possess empathy, it not only positively affects patient treatment, but also promotes nursing work. Communicating with patients through sincere, gentle words and eye contact helps establish a trusting relationship, alleviate negative emotions, stimulate positive emotional experiences, and improve psychological resilience [2]. As a therapeutic factor, empathy can effectively promote nurse–patient communication, playing an important role in improving tense nurse–patient relationships and preventing occupational burnout [3]. Nursing students, as the new force and reserve of the nursing workforce, require attention to the development of their empathy. However, previous empathy assessments have mainly relied on self-report scales (such as the Jefferson Scale of Empathy), which are susceptible to social desirability bias and memory errors, making it difficult to objectively capture dynamic behavioral manifestations [4]. Video recording methods can continuously record the subject’s behavior throughout the entire experiment process, thereby revealing the developmental changes of empathy under different situations. Video data help record the context in which specific behaviors are embedded, as well as contents that other data types like verbal expression, emotional display, and body movements cannot easily capture [5]. Video data can capture tacit information and nonverbal expressions that are difficult to present through textual records or interviews. This description preserves the unique advantages of “video data” compared to other information collection methods (text, interviews), uses “tacit information” to correspond to the core connotation of “silent expression,” and supplements “nonverbal expression” to specify how this information manifests, thereby more clearly highlighting the ability of video data to capture indirect and latent information. Therefore, this study aims to break through the limitations of traditional empathy assessments by introducing video analysis methods. Through standardized scenario simulations recording nursing students’ interactive behaviors, combined with multidimensional coding techniques, this study explores the authentic characteristics of their clinical empathy.
2. Subjects and methods
2.1. Research subjects
2.1.1. Video analysis subjects
Using purposive sampling, 26 undergraduate nursing students from a university in Henan Province, who have not yet started clinical internships, were selected as the subjects for video analysis. Inclusion criteria: (1) Currently enrolled full-time undergraduate nursing students at a university in Henan Province. (2) Have not yet participated in clinical internships. (3) Possess normal verbal expression and comprehension abilities and can independently complete nurse–patient communication tasks in simulated scenarios. (4) Voluntarily participate in this study, have signed informed consent forms, understand the study’s purpose and procedures, and are willing to cooperate with interactions in the simulated scenarios. Exclusion criteria: (1) Those unable to complete the simulated scenario interactions due to hearing, speech, or cognitive impairments (e.g., severe stuttering, mental illness). (2) Students who voluntarily withdraw during the research process. To ensure sample homogeneity and data integrity, subjects were anonymized using a four-digit code consisting of “grade + sequence number.” This study has been approved by the Medical Ethics Committee of the First Affiliated Hospital of Henan University of Science and Technology, approval number 2023-0067.
2.2. Research methods
2.2.1. Data collection
Filming was conducted using digital equipment, with cameras placed in the room in advance to ensure a panoramic view capturing the subjects’ actions, responses, and behaviors within the filming area. Data selection criteria were as follows: (1) Videos without background noise or shaking, with clear and discernible sound. (2) Exclusion of footage unrelated to the study theme, unclear speech, poorly organized language, or failure to properly conduct communication. (3) Individual video recordings with a duration longer than 5 minutes.
2.2.2. Video coding analysis
During the simulated scenario demonstrations, researchers recorded the interactions. The recording equipment had a resolution of no less than 1920×1080 pixels and was equipped with an external microphone to ensure clear audio capture. The camera was fixed 1.5 meters directly in front of the simulation ward operation table at a 45° angle, covering the entire nurse–patient interaction area and clearly recording students’ facial expressions and the entire verbal communication process. Three days prior to recording, the simulation ward was set up, including standardized patient positioning and medical equipment arrangement. Participating students conducted rehearsals to familiarize themselves with the filming environment. The video materials were independently coded by two systematically trained researchers according to the “Nursing Simulation Training Behavior Coding Manual,” coding indicators such as nurse–patient communication duration and nonverbal communication behaviors (e.g., eye contact, soothing body gestures). Discrepancies in coding were resolved through discussion to reach consensus.
2.2.3. Video analysis methods
Facial Expression Coding: The Facial Action Coding System (FACS) was used to identify microexpressions exhibited by nursing students during the simulated scenarios, such as slight smiles, frowns, and frequency of eye contact. Speech Emotion Analysis: Praat speech analysis software was employed to extract prosodic features, including pitch and speech rate. Empathy-related keywords were manually annotated, screening for statements in the videos that directly expressed care, and the frequency of these keywords was statistically counted.
2.2.4. Professional preparation
Simulation was first conducted with Standardized Patients (SPs) who were not among the research subjects. Strictly selected SPs underwent rigorous simulation performance training, including at least two rehearsal sessions. To ensure immersion and realism, this study applied simulated makeup techniques: elderly role players wore wigs and elderly clothing, and applied wrinkle latex to their faces to present aging effects. Nurse actors wore professional nurse uniforms. Regarding the setting, all simulation classrooms were arranged to closely resemble real clinical environments. Prior to formal demonstrations, actors ensured the scenes were lifelike and realistic, quickly immersing the research subjects into the scenarios. This approach enhanced the authenticity of participants’ experiences and facilitated accurate recording and subsequent analysis of their responses.
2.3. Statistical analysis
NVivo 22.0 software was used for thematic modeling of the video transcripts, employing a three-level coding process for theme extraction: First-level coding (Open Coding): Key behaviors (e.g., “gently patting the patient,” “asking about pain location”) and emotional expressions (e.g., “using a gentle tone,” “silence or avoidance”) were annotated sentence-by-sentence to generate initial nodes. Second-level coding (Axial Coding): Semantically related initial nodes were categorized and merged to form core dimensions such as “emotional response and connection,” “emotion recognition and understanding,” and “communication barriers and empathy deficits.” Third-level coding (Selective Coding): Through node co-occurrence analysis (e.g., the strength of association between “nonverbal care” and “emotional synchrony”), cross-dimensional themes such as the influence of gender roles and scenario-induced stress effects were distilled, clarifying the logical relationships between core themes and subthemes.
3. Results
3.1. General characteristics of the study subjects
Baseline data showed that females accounted for 62.5% (20/26) of the sample, with a mean age of 20 ± 1.2 years. The subjects’ average Grade Point Average (GPA) was 3.8 ± 0.4, and none had clinical practice experience.
3.2. Thematic analysis of nursing students’ empathy
Based on video analysis results, using NVivo 22.0 for linguistic emotion coding and dual independent behavioral coding (Kappa = 0.87), combined with the aforementioned coding framework for nursing empathy video analysis, the interactive behaviors of nursing students in standardized simulated scenarios were systematically coded. This covered multidimensional behavioral indicators and emotional characteristics including perception, cognition, expression, and action.
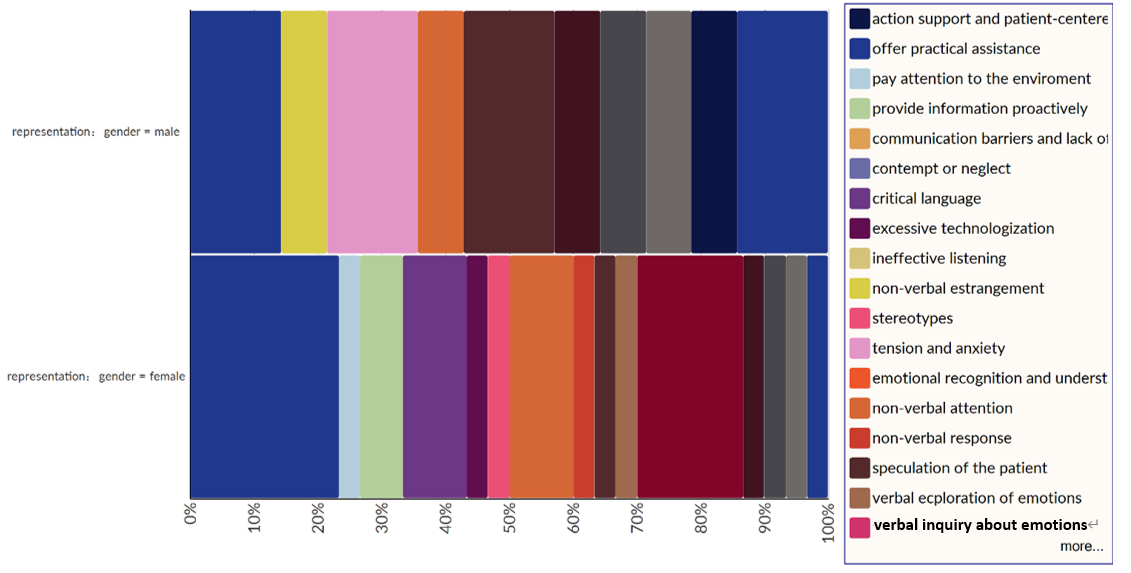
This study proposed three core themes of nursing empathy: emotional response and connection, emotion recognition and understanding, and communication barriers and empathy deficits (see Figure 1).
Under the emotional response and connection dimension, categories included verbal expressions (comfort such as “I understand you,” support such as “We face this together”), nonverbal expressions (caring behaviors like gentle patting or squatting posture, emotional synchrony such as tone matching), and cultural behaviors (objectified care like handing tissues, modest contact like adjusting the patient’s collar).
Under the emotion recognition and understanding dimension, aspects covered perception (nonverbal attention such as eye contact/posture observation, verbal inquiry about emotions) and cognition (inferring the patient’s situation, understanding emotional origins such as “family members crying due to guilt”).
Under the communication barriers and empathy deficits dimension, behaviors included signaling ineffective listening (interrupting conversations, overly technical and mechanical execution of procedures), and attitudinal tendencies (minimizing emotions such as “Don’t think too much,” stereotyping such as “All elderly people have hearing loss”).
3.3. Gender differences in core empathy themes
Regarding emotional response and connection, female nursing students were better at establishing emotional connections through diverse means such as verbal comfort and nonverbal caring behaviors, with a significant advantage particularly in nonverbal caring expressions and emotional synchrony. In emotion recognition and understanding, males and females showed minimal differences in basic abilities, including nonverbal attention at the perceptual level and understanding emotional roots at the cognitive level. In communication barriers and empathy deficits, male nursing students exhibited a relatively higher incidence of issues such as excessive technicality and ineffective listening, reflecting gender-differentiated characteristics in empathy expression and practice (see Figure 1).
(1) Emotional Response and Connection Dimension: Female nursing students demonstrated a relative advantage in emotional connection behaviors, particularly in nonverbal caring expressions (a difference of 45%) and emotional synchrony (a difference of 39%). Nonverbal caring was exemplified in the “Community Clinic” scenario, where N5 (female student) actively supported an elderly person by slightly leaning forward to stay close while gently holding the patient’s elbow (rather than simply pulling), combined with a bending posture to engage in eye-level communication. This posture ensured safety while conveying an attitude of equality and respect. N6 (female student), when inquiring about the elderly person’s pain, maintained a bent posture throughout—even when the patient repeated questions—using stable body language to reinforce the signal “I am listening attentively.” In the “bereaved family” scenario, N1 (female student) used a combination of gentle back stroking and squatting down beside the family member. The squatting posture eliminated the oppressive height difference, while the rhythm of the hand’s light pressure synchronized with the family member’s sobbing, creating a silent emotional resonance. N2 (female student) semi-sat on the floor, embracing the family member with broader but gentle body contact, providing support without intrusion, aligning with the bereaved’s need for “companionship rather than intervention.” Emotional synchrony was shown when addressing a hearing-impaired elderly patient: N5 (female student) did not raise her voice but slowed speech and emphasized keywords (e.g., “brain CT,” “free of charge”), accompanied by hand gestures to aid reception. N7 (female student), when the patient expressed headache, shifted tone from steady to gently concerned, with a slight rising intonation at sentence end (e.g., “Is it intermittent?”), conveying attention to symptoms. In the “bereaved family” scenario, N1’s consoling speech rhythm synchronized with the family’s emotional fluctuations—slowing down and lowering tone when the family cried (“I know it’s really hard now”), then gradually increasing strength as the family calmed (“but we must have the courage to start anew”), avoiding abrupt or forced consolation. N2’s tone incorporated a slight tremor when referring to “the loved one who has not truly left,” echoing the family’s sadness rather than maintaining a mechanical flat tone. The usage rate of female nursing students’ nonverbal caring expressions (67%) was three times that of males (22%), and this coupled with emotional synchrony (58%) formed a reinforcing loop, indicating nonverbal skills as a key target for gender-differentiated training (see Table 1).
|
Behavior Node |
Female Nursing Students |
Male Nursing Students |
Difference |
|
Nonverbal Caring Expression |
67% |
22% |
+45% |
|
Emotional Synchrony |
58% |
19% |
+39% |
|
Verbal Comfort Expression |
52% |
25% |
+27% |
|
Verbal Support Expression |
49% |
31% |
+18% |
|
Personalized Caring Behavior |
43% |
18% |
+25% |
(2) Emotion Recognition and Understanding Dimension: No significant gender differences were found. In the community clinic scenario, male and female nursing students showed no significant difference in recognizing core elderly needs such as pain, examination demands, and hearing impairment. In the bereaved family scenario, both genders similarly understood and responded to core emotions of “sadness” and “pain.” From the subtheme “Emotion Recognition and Understanding,” core indicators such as inferring situations and understanding emotional origins showed no significant stratification between genders. Basic emotional recognition abilities were highly similar between males and females (difference <5%), refuting the stereotype that “women are better at reading social cues.” Cognitive abilities such as emotion recognition and understanding (female 39% vs. male 36%) and nonverbal attention (female 38% vs. male 35%) differed by less than 5%, indicating that gender differences exist only at the expression level rather than perception (see Table 2).
|
Behavior Node |
Female Nursing Students |
Male Nursing Students |
Difference |
|
Nonverbal Attention |
38% |
35% |
+3% |
|
Nonverbal Response |
41% |
37% |
+4% |
|
Emotion Recognition & Understanding |
39% |
36% |
+3% |
(3) Communication Barriers and Empathy Deficits: Male nursing students exhibited a higher risk in this dimension. The probability of communication barriers among male students was significantly higher, with excessive technicality (difference 32%) and ineffective listening (difference 21%) as main risk points. The incidence of excessive technical behavior among male nursing students reached 45%, accompanied by high levels of ineffective listening and emotion minimization (see Table 3).
|
Behavior Node |
Female Nursing Students |
Male Nursing Students |
Difference |
|
Ineffective Listening |
32% |
11% |
+21% |
|
Minimizing or Ignoring Emotions |
28% |
9% |
+19% |
|
Excessive Technicality |
45% |
13% |
+32% |
|
Critical Language |
23% |
8% |
+15% |
|
Nonverbal Alienation |
27% |
12% |
+15% |
|
Stereotyping |
19% |
6% |
+13% |
3.4. Differences in nursing students’ empathy performance across different scenarios
In low emotional load scenarios such as the “Community Clinic,” the completeness of nursing students’ empathy behaviors reached 79%; in high-pressure scenarios such as “Cancer Pain,” completeness dropped to 53%.
Common behaviors across scenarios were mainly reflected in basic caring responses, including: immediate physical support for service recipients (e.g., helping to support or offering a seat—both N1 and N10 prioritized helping elderly patients to sit in the community clinic, while N1 and N4 adopted squatting or semi-sitting postures close to family members in bereavement scenarios); preliminary inquiry into core needs (e.g., asking about pain location like “Where did you fall?” or confirming emotional status like “How are you feeling now?”); and basic soothing actions (e.g., gentle patting, handing tissues—with N1 and N4 using such behaviors to respond to the bereaved family’s sadness). Specialized behaviors diverged significantly according to scenario characteristics:
In the low emotional load “Community Clinic” scenario, empathy behaviors tended toward detailed informational support and adaptive adjustment. For example, N2 proactively moved a stool for an elderly patient and gave detailed explanations of examination items; N3 and N5 assisted when the elderly patient was unable to scan a QR code; N7 used plain language to explain the relationship between osteoporosis and risk of bruising to alleviate concerns; N6 refined pain description by following up with questions like “Is it a dull pain or intermittent?”—reflecting patience in breaking down needs and adaptive responses to the elderly patient.
In high-pressure scenarios such as “Cancer Pain,” empathy behaviors focused more on immediate emotional comfort and sharing of pain. Female nursing students (N1, N3) reinforced emotional connection through “attentive listening” and “continuous companionship,” while male nursing students (N4, N5) directly responded to painful emotions with verbal comfort. Both reduced complex informational output, instead using concise supportive language and physical contact (such as gentle patting or stroking) to convey care, with an emphasis on alleviating the acute emotional impact of severe pain. Detailed behavior comparisons are shown in Table 4.
|
Theme |
Common Behaviors |
Specialized Behaviors |
|
|
Community Clinic |
Emotion |
Helping elderly to sit, asking about pain, mentioning family, bending posture, moderate voice, supporting physically |
Health education, proactive responses, intervention to understand medical history, use of professional terminology and discipline knowledge, emotional guidance |
|
Bereaved Family |
Cognition |
Consoling |
Handing tissues, stroking, gentle patting, wiping tears, squatting |
|
Elderly with Cancer Pain |
Verbal comfort |
Patting, body movements, singing to patients, squatting, handshakes (female nursing students); proposing pain relief measures (male nursing students) |
|
|
Elderly with Diabetic Foot |
Dietary guidance, health education |
Wound inspection, wound care, scheduled disinfection, proactive responses |
|
|
Elderly with Incorrect Use of Crutches |
Supporting, observing, correcting errors |
Assessing leg muscle strength |
|
|
Hypertensive Patients |
Guidance on correct medication use and adherence to prescriptions |
Asking about medical history and daily diet, health education, application of discipline knowledge |
4. Discussion
This study utilized video analysis combined with scenario-based simulation to deeply explore the development and application of empathy in undergraduate nursing students during clinical internships. Such a multidimensional approach holds significant value for improving nursing education quality and enhancing nursing students’ professional competence. For the first time, a standardized video analysis framework was applied to evaluate nursing students’ empathy, capturing numerous nonverbal behaviors (e.g., eye avoidance, brief smiles) that are key empathy indicators often overlooked in previous research.
Among the three core dimensions identified, “emotional response and connection” is the most externally visible behavioral aspect of empathy. It mainly reflects the process by which nursing students establish emotional resonance with service recipients through verbal, nonverbal, and cultural behaviors. Notably, this dimension exhibited significant gender differences, consistent with existing studies on nursing students’ empathic behaviors. This gender disparity aligns with the findings of Ni et al. [6], who pointed out that “female nursing students demonstrate significantly higher sensitivity in emotional expression and bodily empathy, whereas males tend to adopt a ‘problem-solving’ oriented, rational response.” Our study further refines this difference: females’ advantage lies not only in “what to do” (types of nonverbal behaviors) but also “how to do it” (the synchrony between behaviors and others’ emotions). This “refined emotional regulation ability” may be related to cultural expectations in gender role socialization, where females are more attuned to relationship maintenance. Similarly, Hu et al. [7] noted that female nurses are more likely to be rated by patients as “caring” in clinical practice, supporting the clinical continuity of females’ emotional response advantages found in our study. This suggests that nursing education should strengthen nonverbal emotional skills training for male nursing students to compensate for their emotional connection deficits.
The “emotion recognition and understanding” dimension, as the cognitive core of empathy, centers on nursing students’ perception of emotional signals (e.g., nonverbal attention) and interpretation of deeper emotional causes (e.g., inferring situations). This study found no significant gender difference in this dimension, indicating a foundational common empathy ability among nursing students, which challenges the stereotype that “females are better at reading social cues.” Although existing research often emphasizes gender differences in emotion recognition, our findings align with some specialized subfield conclusions. For example, Song et al. [8], in their study on nursing students’ health education abilities, found that “basic judgment of service recipients’ emotional needs” is a core shared competence, with gender differences mainly in “post-recognition responses” rather than recognition itself. This complements our conclusion of “no difference in emotion recognition but differences in expression.” This suggests that emotion recognition and understanding can be taught as a common foundational course in nursing education without gender-differentiated design, while focusing on training the ability to “transform recognition into effective response.”
The “communication barriers and empathy deficits” dimension reflects empathy breakdowns caused by behavioral or attitudinal deviations during interactions. This study found that risk behaviors in this dimension are more concentrated among male nursing students and related to a “technology-first” professional cognitive tendency. This feature shares commonality with studies on behavioral deviations in clinical nurses. Luo et al. [9], in their research on empathy cultivation among novice nurses, mentioned that “imbalance between technical training and emotional communication training leads to interaction barriers,” providing an explanation for communication problems among nursing students in our study. The current intensive technical operation training in nursing education may reinforce a “technology-oriented” cognition especially among male students, which requires correction through integrated “technology + emotion” training.
Gender differences and commonalities in nursing students’ empathy: Gender roles and social atmosphere profoundly influence individual emotional responses and regulation during socialization. Females generally exhibit distinct, deeper traits in emotional response and regulation compared to males. Our findings show that female nursing students are typically more skilled at employing verbal and physical contact in emotional expression, while male students tend to express empathy through actions and are less likely to overtly show emotions. This difference is pronounced in clinical internships; for example, when facing elderly cancer patients in pain, female students may soothe with gentle words and light pats, whereas male students might focus more on practical assistance such as repositioning to alleviate pain. Understanding and respecting these differences is fundamental to building harmonious nurse-patient relationships. Future nursing education should tailor approaches based on male and female nursing students’ characteristics, guiding mutual learning and maximizing respective strengths to enhance overall empathy levels. Gender-differentiated training programs could be developed accordingly.
Reasons for differences in nursing students’ empathy behaviors across different scenarios and intervention pathways: This study found that the completeness of nursing students’ empathy behaviors in low emotional load scenarios such as the “Community Clinic” (79%) was significantly higher than in high-pressure scenarios such as “Cancer Pain” (53%). This difference is closely related to the intensity of cognitive load imposed by the scenario and the limitations of existing training models.
On one hand, the multidimensional stimuli in high-pressure scenarios occupy emotional response resources. In scenarios such as “Cancer Pain” and “Consoling Bereaved Families,” patients’ intense emotional expressions (e.g., crying, groaning), complex clinical information (e.g., multiple overlapping symptoms), and potential risk signals (e.g., vital sign fluctuations) generate high cognitive load. This causes nursing students to prioritize attention toward technical tasks (e.g., administering pain relief measures, conducting clinical assessments), thereby compressing the psychological space available for emotional responses. This “cognitive resource competition” phenomenon aligns with the psychological “attention allocation theory,” which posits that when individuals face multiple task demands, they prioritize high-priority tasks (e.g., crisis management) and delay or simplify secondary tasks (e.g., emotional expression).
On the other hand, current nursing education lacks empathy training designs that account for scenario gradients. Existing empathy training for nursing students primarily utilizes standardized simulation scenarios (e.g., routine standardized patient interviews) [10], without layered training based on the “emotional and technical” dimensions. This results in nursing students lacking specialized competence to integrate “technical operations and emotional care” simultaneously in high-pressure scenarios.
5. Limitations and prospects
This study’s six standardized simulated scenarios did not include complex settings such as pediatrics and emergency care. Pediatric patients (e.g., crying children, anxious parents) and emergency environments (e.g., sudden onset of illness, high time pressure) place special demands on nursing students’ empathetic performance. The existing scenarios (e.g., community clinic, cancer pain) cannot fully cover these high-complexity, high-emotional-load clinical contexts, which may limit the applicability of the findings to diverse clinical situations.
In addition, although video analysis can capture students’ behavioral and verbal characteristics, it still has technical limitations: it cannot precisely capture patients’ subtle facial expressions (e.g., frowning, slight tremors indicating potential emotional states) and cannot fully reproduce the implicit atmosphere in a scene (e.g., tension, suppressed emotional pressure). These missing elements are crucial for understanding the dynamic responses of nursing students’ empathy and may result in the omission of some interaction details in emotional exchanges.
6. Conclusion
This study used video analysis to systematically code and analyze the interactive behaviors of 26 pre-internship undergraduate nursing students in six standardized simulated scenarios. For the first time, it constructed an empathy assessment framework for nursing students based on video recordings, distilling three core themes: emotional response and connection, emotional recognition and understanding, and communication barriers with empathy deficits. The study also revealed gender differences in empathy performance and behavioral variation patterns across different scenarios.
The results not only provide the nursing education field with a quantifiable and objective empathy assessment tool—overcoming the limitations of traditional self-report scales—but also extract concrete behavioral indicators that offer clear training targets. For example, the advantage of female nursing students in nonverbal expressions of care and emotional synchrony can be used as model cases for group learning; meanwhile, the problem-solving orientation and over-technification tendency of male nursing students suggest the need to strengthen training in emotional expression skills and the integration of “technical–emotional” competencies. Additionally, the observed differences in empathy behavior completeness across scenarios provide empirical support for developing layered and graduated simulation training systems.
Although this study is limited by its scenario coverage and the inability of video technology to capture all implicit information, the video analysis method explored here opens a new path for empathy research in nursing students. In the future, more diverse simulated scenarios (e.g., pediatrics, emergency care) can be incorporated, along with more advanced emotion recognition technologies (e.g., synchronized physiological signal collection) to deepen understanding of the dynamic development mechanisms of empathy in nursing students. It is also recommended that nursing educators integrate the core behavioral indicators identified in this study into teaching practice, design targeted gender-differentiated training programs and scenario-tiered training modules, and incorporate systematic video feedback technology into empathy courses. This will help effectively improve nursing students’ ability to apply empathy in clinical practice, lay a solid foundation for building harmonious nurse–patient relationships, and enhance the quality of nursing services.
References
[1]. Zheng, R. C., & Li, Z. H. (2006). History and current status of empathy research.Chinese Journal of Mental Health, (4), 277–279.
[2]. Xiao, X., He, X. F., & Wang, X. Y. (2022). Effects of precision nutrition therapy combined with empathetic nursing on nutritional status and psychological resilience in patients undergoing laparoscopic radical resection of colorectal cancer.Journal of North Sichuan Medical College, 37(6), 820–824.
[3]. Zhang, Z. H. (2013). Research progress on the role of empathy in nurse-patient communication.Journal of Clinical Nursing, 12(6), 51–53.
[4]. Jiang, T., Wan, X. Y., & Liu, Y. Y. (2015). Reliability and validity of the Chinese version of Jefferson Scale of Empathy (medical student version).Journal of Sichuan University (Medical Edition), 46(4), 602–605.
[5]. Lv, X. L., Zhu, X., & Fu, S. Z. (2022). Video research methodology: Opening new avenues in public administration research.Public Administration Review, 15(6), 173–195, 200.
[6]. Ni, F. H., Wang, X. L., & Xu, C. (2008). Investigation and analysis of empathy characteristics among three-year nursing students in our hospital.Journal of Qiqihar Medical University, 29(22), 2753–2754.
[7]. Hu, Y. N., Ge, G. Q., & Zou, H. H. (2022). Current status and influencing factors of humanistic care ability among nursing staff in Zhengzhou.Chinese Journal of Health Psychology, 30(9), 1326–1331.
[8]. Song, J. Y., Liu, R. R., & Tang, Y. M. (2025). Influencing factors of health education ability among nursing students in higher education institutions.Continuing Medical Education, 39(5), 129–134.
[9]. Luo, S. H., Zhang, C. F., & Yin, C. X. (2022). Evaluation of the effect of sensibility quality workshops on empathy cultivation in new nurses.Continuing Medical Education, 36(1), 61–64.
[10]. Dai, X. (2022). Progress in the application of standardized patients in clinical nursing education.China Urban and Rural Enterprise Health, 37(6), 76–78.
Cite this article
Ma,J.;Zhang,A. (2025). Undergraduate nursing students’ empathy before clinical internship: a video recording-based analysis. Advances in Social Behavior Research,16(6),59-66.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Journal:Advances in Social Behavior Research
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Zheng, R. C., & Li, Z. H. (2006). History and current status of empathy research.Chinese Journal of Mental Health, (4), 277–279.
[2]. Xiao, X., He, X. F., & Wang, X. Y. (2022). Effects of precision nutrition therapy combined with empathetic nursing on nutritional status and psychological resilience in patients undergoing laparoscopic radical resection of colorectal cancer.Journal of North Sichuan Medical College, 37(6), 820–824.
[3]. Zhang, Z. H. (2013). Research progress on the role of empathy in nurse-patient communication.Journal of Clinical Nursing, 12(6), 51–53.
[4]. Jiang, T., Wan, X. Y., & Liu, Y. Y. (2015). Reliability and validity of the Chinese version of Jefferson Scale of Empathy (medical student version).Journal of Sichuan University (Medical Edition), 46(4), 602–605.
[5]. Lv, X. L., Zhu, X., & Fu, S. Z. (2022). Video research methodology: Opening new avenues in public administration research.Public Administration Review, 15(6), 173–195, 200.
[6]. Ni, F. H., Wang, X. L., & Xu, C. (2008). Investigation and analysis of empathy characteristics among three-year nursing students in our hospital.Journal of Qiqihar Medical University, 29(22), 2753–2754.
[7]. Hu, Y. N., Ge, G. Q., & Zou, H. H. (2022). Current status and influencing factors of humanistic care ability among nursing staff in Zhengzhou.Chinese Journal of Health Psychology, 30(9), 1326–1331.
[8]. Song, J. Y., Liu, R. R., & Tang, Y. M. (2025). Influencing factors of health education ability among nursing students in higher education institutions.Continuing Medical Education, 39(5), 129–134.
[9]. Luo, S. H., Zhang, C. F., & Yin, C. X. (2022). Evaluation of the effect of sensibility quality workshops on empathy cultivation in new nurses.Continuing Medical Education, 36(1), 61–64.
[10]. Dai, X. (2022). Progress in the application of standardized patients in clinical nursing education.China Urban and Rural Enterprise Health, 37(6), 76–78.