







1. Introduction
Since the inception of the clinical system, there has been a constant drive to make the process better so that it is quicker and more effective overall. Traditional operations have long been standardized and in demand thanks to the advancements in medicine. It has several benefits, including being effective in treating a wide range of medical conditions, enabling surgeons to directly visualize and manipulate organs and tissues, being quick to perform in emergencies, and perhaps most importantly, the fact that surgeons are highly trained and experienced in traditional surgical techniques, which gives them greater decision-making flexibility and better judgment in the event of accidents. On the other hand, inevitably doctors may also make mistakes during practice due to hand trembling, emotional affection, also their own mental and physical health. Because of the complexity of surgery and the need for good safety, especially for complex surgery with great precision, how doctors treat patients has a big impact on the results. The level of uncertainty kept upsetting the researchers, and it felt like there was no other way to fix the issues besides gaining expertise to prevent mistakes.
With the debut of the first surgical robot, the PUMA 560, in 1985, the field of clinical medicine experienced a revolutionary advancement. The use of robotics in surgical procedures began with this surgery for a brain biopsy. To reduce the effect of hand tremors on surgical precision, robotic surgery was introduced as one of its main goals. This innovative application of robotic technology paved the way for subsequent developments in robotic-assisted surgery. In the 1990s, IBM and Integrated Surgical Solutions created ROBODOC [1]. ROBODOC was successfully used in human surgery in 1992. In later years, researchers created the Da Vinci surgical system, AESOP, and Zeus surgical system, which greatly promoted the development of medical technology.
Many kinetic models have been proposed and optimized because of technological advancements in software controls and algorithms. With advanced technology, people may further reduce the risk of surgical errors. The Hisense Computer-Aided Surgery System (CAS) is a precision surgical solution to help doctors with preoperative accurate planning, intraoperative reference, and postoperative evaluation. It is supported by the nation's 12th Five-Year Support Plan and is based on enhanced CT images for in-depth data mining, accurate restoration of organs, lesions, and peripheral vascular systems.
The robotic arm is an automated mechanical tool that can be programmed to behave like a human arm and can carry out a range of activities with extreme accuracy and efficiency. It has been used in manufacturing, logistics, and other industries. Researchers' visions have been sparked by robotic arms' impressive performance. Nowadays, academics are interested in how to enhance dynamic models and algorithms in the therapeutic sector and make wise use of artificial intelligence and new technologies.
Fortunately, since the technological revolution, medical device research has advanced significantly. The accuracy demands of the doctor's manual operation can be decreased by the medical device's precise control.
In this research, hardware will be introduced including the basic components of surgical robotic arms and the kinetic dynamic functions being used during moments, and the software — in terms of the active contour models for tracking nodules and the method for localization. The application of clinical technologies and the use of a robotic arm during the operation will also be elaborated. Using the data at hand, anticipation and estimation would be made into the prospect of the project from its current utilization.
2. Software and algorithms
2.1. Raspberry Pi
From figure 1, the Raspberry Pi was presented. Raspberry Pi was founded in UK, as a line of compact single-board computers. The purpose of these credit-card-sized computers is to further computer science education and offer enthusiasts, students, and developers an affordable and accessible platform to experiment with hardware and software projects. To test the possibility of auto-tumor removal surgeries, a robotic arm with six degrees of freedom will be operated via Raspberry Pi in this study, hoping to encourage the detection and removal of a potential tumor while preserving more medical resources for other patients.


(1)Raspberry Pi (2) Arm Pi
Figure 1. Hardware used in experiment.
2.2. Medical Image Analysis
Clinical medicine today uses various AI-driven technologies, such as Medical Imaging Analysis, Risk Assessment, Personalized Treatment Planning, Decision Support, Computer-Assisted Diagnostics, and Surgical Navigation, to help surgeons before, during, and after surgery. With the help of AI, surgical procedures may now be virtually simulated, giving the surgeon the opportunity to practice different scenarios and gain expertise. This method has received recognition for its usage in education. Instance Segmentation, Atlas-based Segmentation, and Active Contour Models will be featured extensively in this study to highlight the application of Medical Imaging Analysis in locating and eliminating tumors.
2.2.1. Vectors
Radiation has become more conformal since the introduction of cutting-edge beam delivery methods including stereotactic ablative radiotherapy (SABR), volumetric modulated arc therapy (VMAT), and intensity-modulated radiotherapy (IMRT) [2]. By producing a highly conformal dose distribution that is tightly contoured to tumour volume and lowering the quantity of normal tissue exposed to radiation, these approaches have considerably improved routine practice. With the best localization methods, surgeons will have a wide range of options for clearly detecting these nodules and will have the best chance of preserving as much lung tissue as possible. The surgical localisation of lung nodules, however, may be challenging in several ways.
The location and surgical resection of tumours are significantly influenced by several tumour-related variables. The nodule's size, proximity to the pleural surface, nature (whether it is solid, ground glass, or mixed), any concomitant structural lung diseases, the presence of anthracitic pigment on the lung surface, and the presence of pleural adhesions are some of these factors [3]. To guarantee a successful and accurate procedure, each of these elements must be carefully considered and evaluated during the surgical planning process. Image-guided radiation (IGRT) (8–11) improves the accuracy and precision of dose placement to the target volumes and the surrounding normal tissues by using imaging systems for radiotherapy devices to direct the treatment [4]. It is now possible to control organ movement during treatment and to be aware of the location of the irradiated target organ thanks to the development of IGRT. A demonstration of object detection and tracking using colour is shown in Figure 2.
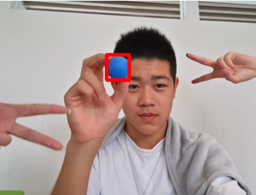


(1) Tracking colour blue (2) Tracking colour red (3) Tracking colour black
Figure 2. Colour tracking demonstration.
2.2.2. Active Contour Models
An item shape can be discerned from a potentially noisy 2D image using the active contour model, often known as snakes. A snake is an energy-minimizing, deformable spline that is pulled toward object outlines by constraint and image forces as well as internal forces that prevent deformation. Images only allow for integration over finite time steps and have a finite resolution, therefore, discrete approximations must be used to implement snakes practically [5].
\( E_{snake }^{*}≈\sum _{1}^{n} {E_{snake }}({\bar{v}_{i}}) \)
\( F_{snake }^{*}≈-\sum _{i=1}^{n} ∇{E_{snake }}({\bar{v}_{i}}) \)
Adding discrete time to the method can result in updates that move the snake away from the minima it is drawn to, which can then lead to oscillations around the minima or the discovery of a new minima. This can be prevented by adjusting the time step so that the picture forces limit it to a step size of no more than a pixel. The internal energies, however, will predominate the update in low-energy areas. A different option is to normalize the image forces for each step so that they only update the snake by one pixel.
\( {F_{image }}=-k\frac{∇{E_{image }}}{∥∇{E_{image }}∥} \)
The GVF Snake Model, Balloon Model, Diffusion Snakes Model, and Geometric Active Contours are the four main models that should be highlighted. Each has a unique area of expertise.
The standard snake model faces two important problems that the gradient vector flow (GVF) snake model seeks to address: insufficient completion for concave boundaries and when initialized far from minimum. By computing the GVF using the image's gradient information, a vector field is constructed that contains the global image features.
\( {E_{GVF}}=∬μ(u_{x}^{2}+u_{y}^{2}+v_{x}^{2}+v_{y}^{2})+|∇f{|^{2}}|v-∇f{|^{2}}dxdy \)
\( μ{∇^{2}}u-(u-\frac{∂}{∂x}{F_{ext }})(\frac{∂}{∂x}{F_{ext }}(x,y{)^{2}}+\frac{∂}{∂y}{F_{ext }}(x,y{)^{2}})=0 \)
\( μ{∇^{2}}v-(v-\frac{∂}{∂y}{F_{ext }})(\frac{∂}{∂x}{F_{ext }}(x,y{)^{2}}+\frac{∂}{∂y}{F_{ext }}(x,y{)^{2}})=0 \)
This problem can be resolved by solving the Euler equations, where x is a configurable smoothing term.
\( {u_{i+1}}={u_{i}}+μ{∇^{2}}{u_{i}}-({u_{i}}-\frac{∂}{∂x}{F_{ext }})(\frac{∂}{∂x}{F_{ext }}(x,y{)^{2}}+\frac{∂}{∂y}{F_{ext }}(x,y{)^{2}}) \)
\( {v_{i+1}}={v_{i}}+μ{∇^{2}}{v_{i}}-({v_{i}}-\frac{∂}{∂y}{F_{ext }})(\frac{∂}{∂x}{F_{ext }}(x,y{)^{2}}+\frac{∂}{∂y}{F_{ext }}(x,y{)^{2}}) \)
The default external force is replaced with this outcome.
\( F_{ext}^{*}={F_{GVF}} \)
Figure 3 shows object contour detection.
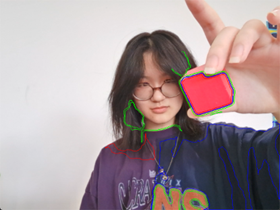


(1) Contouring red cube (2) Contouring blue ball with (3) Contouring blue ball improved program
Figure 3. Contouring display.
3. Hardware and Kinetic Models
3.1. Hardware
Robotic arms have been widely used in surgical research over the past few decades thanks to advancements in information technologies and dynamic algorithms. In order to provide minimally invasive procedures with improved precision, dexterity, and visibility, surgical robotic devices like "Da Vinci" and "Zeus" had been established. End effectors, degrees of freedom shown in Figure 4, and kinetic mechanisms all play a significant part in the design of robotic arms because of their tight ties to system performance. We would like to use the da Vinci Surgical System which represents the significant advancement in field of robotic-assisted surgery and yet provides numerous benefits to both surgeons and patients from its function.
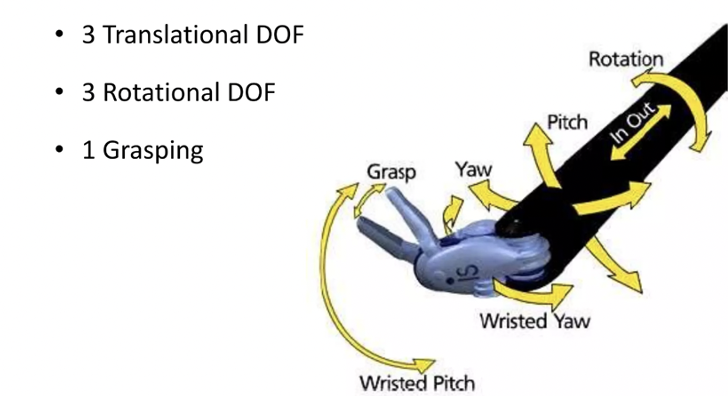
Figure 4. 7 Degrees of freedom.
3.1.1. Articulated Robotic Arms
The da Vinci system typically includes four robotic arms, though some models may have additional arms, the robotic arm system typically consists of four arms, three of which are designated for surgical instruments, while the fourth arm is equipped with a camera featuring a magnified vision system. This camera provides the operator with a three-dimensional (3D) view of the surgical site during the procedure.
These robotic arms mimic the structure and movement of a human arm, consisting of multiple linked segments or joints connected by actuators (motors) that allow the arm to move in multiple degrees of freedom (DOF) shown in Figure 5. Common joint types include revolute (rotational) joints and prismatic (linear) joints, the higher the number of joints, the higher the flexibility.
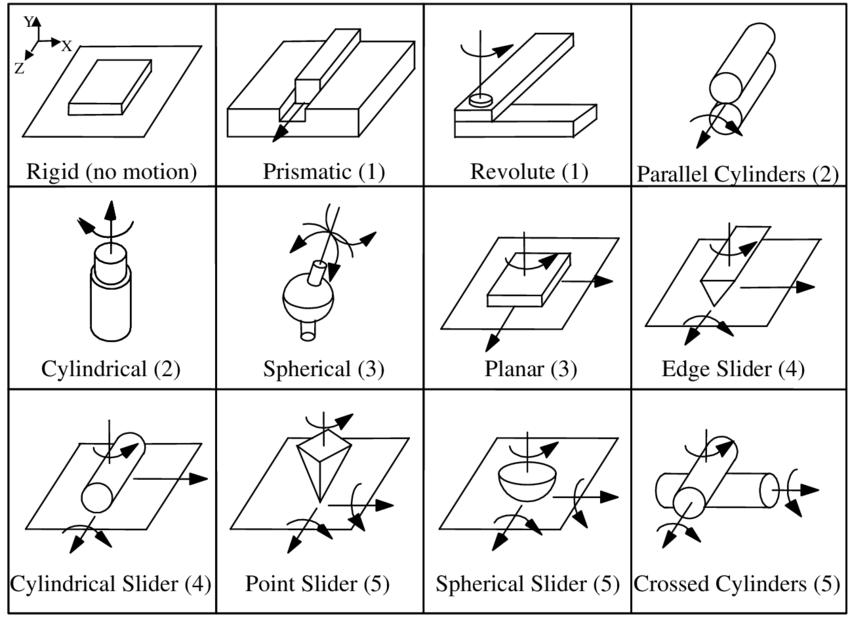
Figure 5. 17 3D Kinematic Joint Types, with the Degrees of Freedom indicated.
3.1.2. End-Effector
The end-effector, a tool or gadget used to interact during surgery, is located at the end of the articulated arm. Various surgical tools, such as forceps, scissors, needle drivers, graspers, and electrocautery tools, among others, can be attached to the end-effector. Figure 6 shows the Da Vinci robotic arm [6]. These instruments are interchangeable and may be swiftly exchanged.
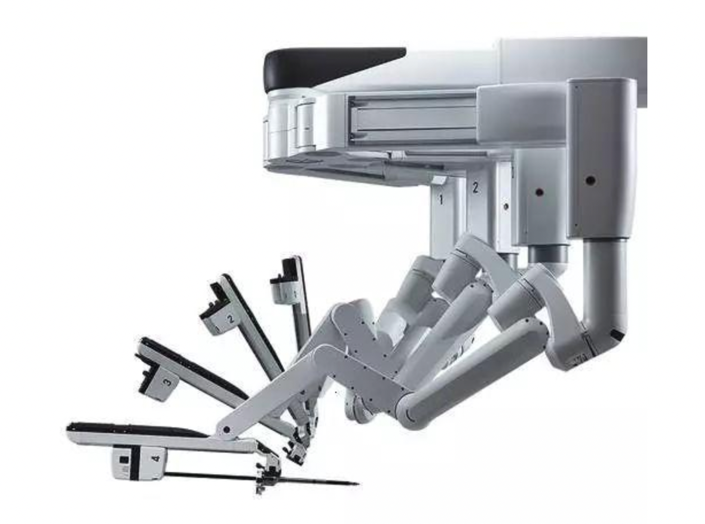
Figure 6. Da Vinci robotic arm.
3.2. Kinematics and Control of the Arm
For the kinematics with articulated robotic arms, it is necessary to solve the forward and inverse kinematics (which entail computing joint angles to determine the end-effector's location). To arrange movements and controls precisely, these calculations are essential.
3.2.1. Theory of Remote Center of Motion (RCM)
RCM is a hypothetical point that the robotic arm revolves around while remaining stationary in space. This fixed point minimizes tissue damage and improves surgical precision by allowing the end-effector to move within the patient's body without producing any translation (motion along the axis) at the point of insertion [7].
The most popular RCM mechanism now is the double-parallelogram technique. As an illustration, the double-parallelogram mechanism is used in the renowned Da Vinci surgical robot to accomplish the remote center of motion. From the basic ideology of the mechanism, Tan and Kong suggested a novel kind of RCM mechanism. As shown in Figure 7, Kong’s system enables the yaw and translation of surgical instruments in 2-DOF [8].
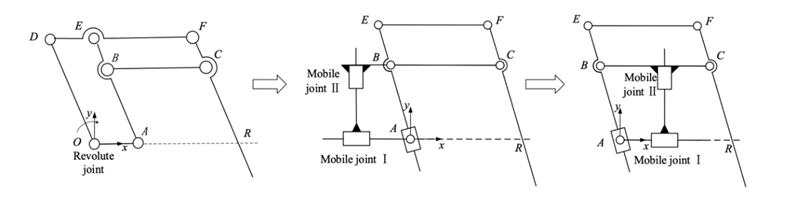
Figure 7. The figure of deduction of planar 2-DOF RCM mechanism.
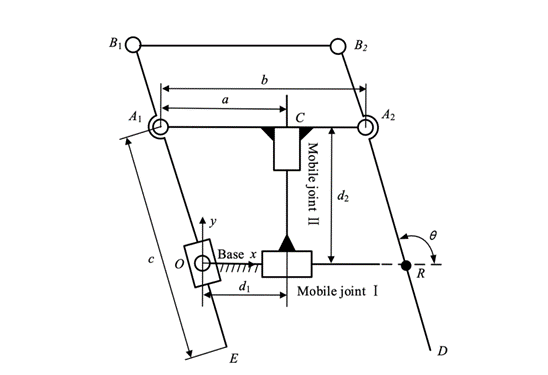
Figure 8. Mechanism of RCM.
3.2.2. The PID
As shown in Figure 9, Proportional-Integral-Derivative [9], or PID, is a commonly used control algorithm to maintain or regulate a desired setpoint in many different sectors and applications. In systems with feedback loops, where the control input (actuator) is changed according to the discrepancy between the intended setpoint and the actual system output (process variable), PID control is especially effective [10].
The three terms In the PID control algorithm are as follows:
The proportional term is inversely proportional to the current difference between the process variabl’'s setpoint and actual value. It prompts the controller to react in proportion to the erro’'s severity. The control effort to fix the problem increases with the size of the error. This phrase offers a prompt response to any alteration in the error signal.
The integral term considers the total number of prior mistakes across time. It assists in removing any steady-state inaccuracy that might develop because of outside disruptions or innate system bias. With the help of the integral term, the system is brought to the desired setpoint by eradicating accumulated error over time.
The derivative term takes the erroneous signa’'s rate of change into account. Future error trends are anticipated, and the syste’'s response is dampened, lowering overshooting and oscillations. The derivative term makes the control system more stable.
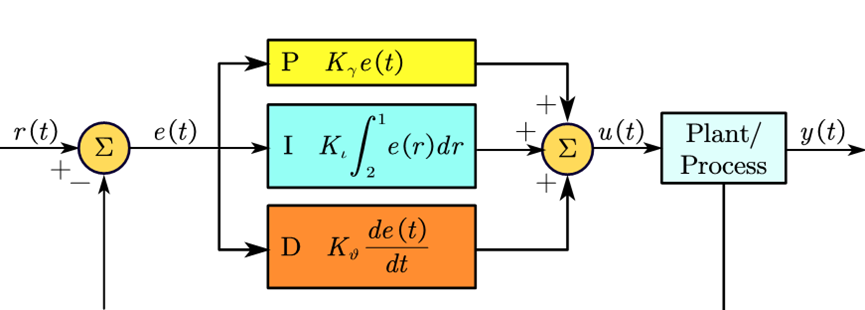
Figure 9. A PID controller.
The PID control algorithm combines these three terms to calculate the control output (u(t)) at any given time:
\( u(t)={K_{p}}e(t)+{K_{i}}\int _{0}^{t} e(τ)dτ+{K_{d}}\frac{de(t)}{dt} \)
The system's control effort (output) is denoted by the symbol u(t). The tuning parameters Kp, Ki, and Kd are also referred to as the proportional, integral, and derivative gains, respectively. The error signal at time t (SP - PV) is denoted as e(t). The integral of the error with respect to time (accumulated error) is represented by the notation e(t) dt. The derivative of the error's rate of change is de(t)/dt.
These three control actions are combined by the PID controller into one control signal, which is then applied to the system under control to modify its behavior and move it closer to the target setpoint.
4. Comparison
In comparison to traditional manual surgeries, surgeries involving robotic arm surgery systems often provide a great range of advantages [11].
Robotic arm surgeries are often minimally invasive because they require fewer incisions than conventional open surgeries, which reduces the risk of surgical trauma [12]. Less bleeding, smaller wounds, and a quicker post-operative recovery are possible for patients. To the surgeons, with the support of highly precise robotic arms and cutting-edge image-guidance technology, a more stable operating circumstance is offered and there would be higher levels of surgical precision. With complex procedures, there would be lower chances of errors and boosted success rates. High-definition 3D cameras are frequently used into robotic arm surgery systems, allowing doctors to visualize the operating area more clearly and thoroughly [13]. Better depth perception provided by the 3D image helps surgeons execute surgeries in small place. Robotic arms' flexibility and range of motion make it possible to do some operations that would be difficult or impossible using more conventional techniques. Robotic arm surgery increases the range of procedures that are practical, providing more patients with minimally invasive choices.
Even if technology advancement offered many advantages, there would still be problems to get solved. The primary drawback of surgical robot use would be the high cost of implementation. Research indicates that by the end of 2010, the global market for robot equipment usage, which was less than $5 billion in 2000, is expected to reach $25 billion. Comparing to traditional surgeries, the expense of robotic surgery is a crucial disadvantage since the cost of gadget care and maintenance may place an unaffordable burden on the families of the patients.
In addition, robotic systems rely heavily on technology, including computer software and mechanical components. Any technical malfunctions or software errors could potentially disrupt surgeries or lead to unexpected downtime. The effect of network delay could also affect the progress of surgeries [14], Cybersecurity risks frequently target surgical robotic systems, and if they are not sufficiently protected, they risk being taken advantage of. Hackers might get unauthorized access to the control software for the surgical robotic system and alter its settings or directives. This could result in unintentional motions or actions during surgery, endangering the patient. The information transmitted between the surgeon's console and the robotic arms might be altered by hackers. This can lead to incorrect instrument positioning or control, which would reduce the procedure's accuracy and safety. In a ransomware attack, hackers can shut down the robotic system or encrypt sensitive data, then demand payment in return for restoring access. Such attacks could impede vital medical treatments or postpone scheduled surgery.
5. Conclusion
Until the most recent update, In April 2009, the Da Vinci Xi system was brought into the field. This system brought significant improvements, including enhanced high-definition imaging and a more streamlined design for improved functionality. Additionally, a notable feature of the Da Vinci Xi system is its capability to accommodate a second surgeon console, facilitating surgical training or enabling collaborative procedures involving two surgeons.
To enhance the application of the system, its accessibility should be improved, and its functions could be more comprehensive. Improvements in haptic feedback are expected. Techniques used in surgery depend on manipulating tissue carefully. Open surgery is thought to be impossible without sensory feedback of haptic cues. Robotic surgeons have so far found a way to make up for the reduced haptic input by estimating forces using the increased visual feedback cues, but delicate manipulation may still be hindered. Although purchasing and maintaining surgical robotic systems comes at a high initial cost, as technology develops and demand rises, costs may eventually decline. Additionally, the advantages of fewer post-operative problems, quicker recovery, and shorter hospital stays can reduce the overall cost of healthcare.
The time between the controller and the reactor as well as the robotic arms would move more quickly. Academics from the same field have created a sliding mode control strategy that makes advantage of fuzzy tuning PID sliding mode surfaces. This strategy effectively reduces the chattering produced by the sliding mode controller and improves the stability of the system. The algorithm's completion should result in an improvement in operational efficiency.
With the improvement in technology, telemedicine, and remote surgery will be made possible by surgical robotic arms as high-speed internet and communication technologies evolve. To provide access to specialized medical knowledge in underserved areas and during crises, surgeons will be able to perform operations on patients in remote locales. As an example, from previous research, there was an inland remote surgery tests between Tokyo and Shizuoka, at more than 150 kilometers, were undertaken in 2007. In the experiments, ISDN(2B+D) and ISDN (23B+D) have been utilized because the average round-trip time-delay of control and image using ISDN(2B+D) was 99.8 milliseconds and 676.0 milliseconds, respectively. The control and picture round-trip time delays over ISDN (23B+D) were 35.6 ms and 785.0 ms, respectively. Previous studies have demonstrated the viability of long-distance remote surgery.
The surgical system offers benefits such as being minimally invasive, providing a more stable operating environment with high-definition 3D cameras, and having a greater range of motion. But its usability could be enhanced, and its capabilities could be expanded. If surgical robots are to be fully utilized, component and system downsizing will be necessary. The viability of an intracorporeal robotic device has been shown, and work in this direction is continue. To improve present design concepts for clinical application, much more work is needed.
Due to the differences in equipment, simulations would have limitations. The more specialized and field-specific professional surgical robotic arms could result in a data mistake as the difference in operation method and device might be escalated. To further increase the effectiveness of surgeries, future research might focus on the development of communication technologies and tactile feedback for surgical robots.
Authors Contribution
All the authors contributed equally, and their names were listed in alphabetical order.
References
[1]. Pransky, J. (1997). ROBODOC‐surgical robot success story. Industrial Robot: An International Journal, 24(3), 231-233.
[2]. Zhao, W., Shen, L., Islam, M. T., Qin, W., Zhang, Z., Liang, X., ... & Li, X. (2021). Artificial intelligence in image-guided radiotherapy: a review of treatment target localization. Quantitative Imaging in Medicine and Surgery, 11(12), 4881.
[3]. Bawaadam, H., Benn, B. S., Colwell, E. M., Oka, T., & Krishna, G. (2023). Lung Nodule Marking With ICG Dye–Soaked Coil Facilitates Localization and Delayed Surgical Resection. Annals of Thoracic Surgery Short Reports.
[4]. Antoniou, G. A., Riga, C. V., Mayer, E. K., Cheshire, N. J., & Bicknell, C. D. (2011). Clinical applications of robotic technology in vascular and endovascular surgery. Journal of vascular surgery, 53(2), 493-499.
[5]. Kass, M., Witkin, A., & Terzopoulos, D. (1988). Snakes: Active contour models. International journal of computer vision, 1(4), 321-331.
[6]. Penza, V., De Momi, E., Enayati, N., Chupin, T., Ortiz, J., & Mattos, L. S. (2017). EnViSoRS: Enhanced vision system for robotic surgery. A user-defined safety volume tracking to minimize the risk of intraoperative bleeding. Frontiers in Robotics and AI, 4, 15.
[7]. Dehghani, M., Moghadam, M. M., & Torabi, P. (2017). Analysis, optimization and prototyping of a parallel RCM mechanism of a surgical robot for craniotomy surgery. Industrial Robot: An International Journal, 45(1), 78-88.
[8]. Shi, H., Liang, Z., Zhang, B., & Wang, H. (2023). Design and Performance Verification of a Novel RCM Mechanism for a Minimally Invasive Surgical Robot. Sensors, 23(4), 2361.
[9]. Li, Y., Ang, K. H., & Chong, G. C. (2006). PID control system analysis and design. IEEE Control Systems Magazine, 26(1), 32-41.
[10]. Tian, X., & Xu, Y. (2020). Low delay control algorithm of robot arm for minimally invasive medical surgery. IEEE Access, 8, 93548-93560.
[11]. Lanfranco, A. R., Castellanos, A. E., Desai, J. P., & Meyers, W. C. (2004). Robotic surgery: a current perspective. Annals of surgery, 239(1), 14.
[12]. Hockstein, N. G., Nolan, J. P., O'Malley Jr, B. W., & Woo, Y. J. (2005). Robotic microlaryngeal surgery: a technical feasibility study using the daVinci surgical robot and an airway mannequin. The Laryngoscope, 115(5), 780-785.
[13]. Taylor, G. W., & Jayne, D. G. (2007). Robotic applications in abdominal surgery: their limitations and future developments. The International Journal of Medical Robotics and Computer Assisted Surgery, 3(1), 3-9.
[14]. Arata, J., Takahashi, H., Pitakwatchara, P., Warisawa, S. I., Tanoue, K., Konishi, K., ... & Hashizume, M. (2007, April). A remote surgery experiment between Japan and Thailand over Internet using a low latency CODEC system. In Proceedings 2007 IEEE international conference on robotics and automation (pp. 953-959). IEEE.
Cite this article
Wang,X.;Weng,S.;Xie,Z. (2024). Artificial intelligence in clinical applications. Applied and Computational Engineering,48,96-105.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Signal Processing and Machine Learning
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Pransky, J. (1997). ROBODOC‐surgical robot success story. Industrial Robot: An International Journal, 24(3), 231-233.
[2]. Zhao, W., Shen, L., Islam, M. T., Qin, W., Zhang, Z., Liang, X., ... & Li, X. (2021). Artificial intelligence in image-guided radiotherapy: a review of treatment target localization. Quantitative Imaging in Medicine and Surgery, 11(12), 4881.
[3]. Bawaadam, H., Benn, B. S., Colwell, E. M., Oka, T., & Krishna, G. (2023). Lung Nodule Marking With ICG Dye–Soaked Coil Facilitates Localization and Delayed Surgical Resection. Annals of Thoracic Surgery Short Reports.
[4]. Antoniou, G. A., Riga, C. V., Mayer, E. K., Cheshire, N. J., & Bicknell, C. D. (2011). Clinical applications of robotic technology in vascular and endovascular surgery. Journal of vascular surgery, 53(2), 493-499.
[5]. Kass, M., Witkin, A., & Terzopoulos, D. (1988). Snakes: Active contour models. International journal of computer vision, 1(4), 321-331.
[6]. Penza, V., De Momi, E., Enayati, N., Chupin, T., Ortiz, J., & Mattos, L. S. (2017). EnViSoRS: Enhanced vision system for robotic surgery. A user-defined safety volume tracking to minimize the risk of intraoperative bleeding. Frontiers in Robotics and AI, 4, 15.
[7]. Dehghani, M., Moghadam, M. M., & Torabi, P. (2017). Analysis, optimization and prototyping of a parallel RCM mechanism of a surgical robot for craniotomy surgery. Industrial Robot: An International Journal, 45(1), 78-88.
[8]. Shi, H., Liang, Z., Zhang, B., & Wang, H. (2023). Design and Performance Verification of a Novel RCM Mechanism for a Minimally Invasive Surgical Robot. Sensors, 23(4), 2361.
[9]. Li, Y., Ang, K. H., & Chong, G. C. (2006). PID control system analysis and design. IEEE Control Systems Magazine, 26(1), 32-41.
[10]. Tian, X., & Xu, Y. (2020). Low delay control algorithm of robot arm for minimally invasive medical surgery. IEEE Access, 8, 93548-93560.
[11]. Lanfranco, A. R., Castellanos, A. E., Desai, J. P., & Meyers, W. C. (2004). Robotic surgery: a current perspective. Annals of surgery, 239(1), 14.
[12]. Hockstein, N. G., Nolan, J. P., O'Malley Jr, B. W., & Woo, Y. J. (2005). Robotic microlaryngeal surgery: a technical feasibility study using the daVinci surgical robot and an airway mannequin. The Laryngoscope, 115(5), 780-785.
[13]. Taylor, G. W., & Jayne, D. G. (2007). Robotic applications in abdominal surgery: their limitations and future developments. The International Journal of Medical Robotics and Computer Assisted Surgery, 3(1), 3-9.
[14]. Arata, J., Takahashi, H., Pitakwatchara, P., Warisawa, S. I., Tanoue, K., Konishi, K., ... & Hashizume, M. (2007, April). A remote surgery experiment between Japan and Thailand over Internet using a low latency CODEC system. In Proceedings 2007 IEEE international conference on robotics and automation (pp. 953-959). IEEE.