







1. Introduction
China is grappling with a severe aging population, coupled with an increasing focus on stroke-related diseases. Consequently, research on wearable lower limb exoskeleton robots becomes particularly important. Wearable lower limb exoskeleton robots represent a type of rehabilitation robot that not only saves a considerable amount of human and material resources but also provides standardized and repetitive rehabilitation training, alleviating the physical stress on rehabilitation physicians.
Recent studies indicate that the structural configuration and human-machine interaction strategies of lower limb exoskeleton robots are two critical areas of current research. Substantial progress has been made in the structural configuration, leveraging the plasticity of the human brain. More accurate and timely rehabilitation training benefits the neural reorganization and compensation within the patient’s brain, thereby increasing survival rates and the probability of recovering motor functions.
As the “second skeleton” of the human body, exoskeleton robots employ an interdisciplinary approach combining engineering and medicine to provide specific assistance to patients in various situations, such as specialized training in strength, stability, and core strength. Rehabilitation robots enhance the coordination of bodily movements, alleviate obstacles caused by brain damage to movement, and achieve optimal therapeutic effects. Rehabilitation training comes in various forms, including active and passive modes. In the active mode, there are four subtypes: active assistance, active, and active resistance. Rehabilitation devices can be categorized as active, passive, or hybrid power devices, and the driving methods include electric, pneumatic, and hydraulic drives. In conclusion, research on lower limb exoskeleton robots plays a pivotal role in rehabilitation.
2. Current Status of Lower Limb Exoskeleton Rehabilitation Robots: Domestic and International Research
2.1. International Lower Limb Exoskeleton Rehabilitation Robots
In recent years, the development of medical exoskeleton robots has progressed rapidly, as illustrated in Figure 1, with the emergence of numerous high-performance lower limb exoskeleton robots.
Vanderbilt University in the United States, in collaboration with Parker Hannifin company, developed the lightweight exoskeleton robot Indego [1]. This robot is primarily used for the rehabilitation training of patients who have lost walking ability due to spinal cord injuries or strokes. It assesses the motor capabilities of paralyzed or hemiplegic patients and provides assistance in walking. EksO GT, developed by Ekso Bionics in the United States, boasts a faster processor and a powerful software system compared to traditional lower limb exoskeleton robots.
In 2019, the wearable exoskeleton robot Exo-H3 was unveiled, a joint effort of the Spanish company Technaid and the Spanish National Research Council’s Biomedical Engineering Group [2]. This robot features a flexible and lightweight structural framework and adopts an open-source programming architecture, allowing algorithm modifications based on individual patient differences and the use of different control strategies. Additionally, Harvard University has developed a flexible pneumatic wearable exoskeleton robot.
Swiss medical equipment company Hocoma, in collaboration with Zurich Balgrist in 1999, produced the Lokomat, the first fully automated gait estimation training system for suspended lower limb exoskeleton rehabilitation robots [3]. This device, containing only two actively driven degrees of freedom, controls the movements of the hip and knee joints. During rehabilitation training, the patient’s thighs and legs are secured to the rehabilitation robot to assist in standing, with adjustments to ankle joint parameters made based on patient comfort. Lokomat utilizes algorithms such as proportional-derivative control and impedance control to achieve both active and passive rehabilitation training. However, during training, the ground reaction force on the patient’s lower limbs is insufficient, limiting its rehabilitation effectiveness. Additionally, the device is costly with limited rehabilitation benefits.
In 2006, the German company Woodway introduced the lokohelp system, comprising a treadmill, Pedago gait machine, and a suspension unloading device [4]. Based on the LOkoSation device, this system standardizes and constrains rehabilitation metrics such as step frequency, stride, range of motion, and exercise intensity. It periodically conducts precise and extensive rehabilitation training to stimulate proprioceptive sensation in the quadriceps, enhance user-initiated movements, reinforce muscle memory, and ultimately restore the user’s motor abilities. However, the lokohelp system has challenges in adapting to users of different body shapes, leading to prolonged matching adjustment times, increased workload for rehabilitation therapists, and issues related to chest compression and impaired breathing due to suspension binding.
Israeli company ReWalk developed the ReWalk Assistive Rehabilitation Walking Robot [5], named after the company itself. This type of robot, composed of motors, batteries, and a noise system, stands out for its remote interaction system. By sending walking commands through a controller, it facilitates sitting-to-standing rehabilitation training, belonging to the active assistance form of training mode. This system avoids the consecutive walking program on the same leg, providing excellent protection for the patient’s lower limbs. Research and clinical experiments associated with ReWalk indicate that most wearers can achieve walking functionality in urban or community settings, contributing to pain relief, spasm alleviation, improved digestion, and the absence of adverse reactions such as falls or disruptions in autonomous reflexes during training.
HAL, developed by Tsukuba University in Japan, is an assistive walking rehabilitation robot [6] featuring an exoskeleton framework, sensors, and a controller. It progressively enhances the mobility of chronic stroke patients during training, facilitating gradual recovery. In HAL’s mechanical structure, the exoskeleton framework supports and stabilizes, sensors detect the patient’s electromyographic signals and gravitational signals, and the controller is responsible for automatic driving and dynamic assistance, ensuring clear hierarchy without interference. Notably, HAL breaks free from treadmill limitations, increasing the freedom of rehabilitation robot training.

Figure 1. International Lower Limb Exoskeleton Rehabilitation Robots, (a) Indego Exoskeleton Robot; (b) Exo-H3 Wearable Exoskeleton Robot; (c) Lokomat Suspended Lower Limb Exoskeleton Rehabilitation Robot; (d) LOkoSation Device; (e) ReWalk Assistive Rehabilitation Walking Robot; (f) HAL Assistive Walking Rehabilitation Robot.
Picture source:
(a)https://image.so.com/view?q=indego%E5%A4%96%E9%AA%A8%E9%AA%BC%E6%9C%BA%E5%99%A8%E4%BA%BA&src=tab_www&correct=indego%E5%A4%96%E9%AA%A8%E9%AA%BC%E6%9C%BA%E5%99%A8%E4%BA%BA&ancestor=list&cmsid=d0a4bf25ef5a6ca45c5b8efd0c2e07a0&cmras=6&cn=0&gn=0&kn=0&crn=0&bxn=0&fsn=60&cuben=0&pornn=0&manun=0&adstar=0&clw=256#id=6af6b21e6899d1aa1c77f096ab32d8c4&currsn=0&ps=60&pc=60
(b)https://www.bio-equip.com/show1equip.asp?equipid=4162720
(c)https://image.so.com/view?q=Lokomat&src=tab_www&correct=Lokomat&ancestor=list&cmsid=19ae4be3d4d6e15c4a82634d700d8ee6&cmras=0&cn=0&gn=0&kn=0&crn=0&bxn=0&fsn=60&cuben=0&pornn=0&manun=0&adstar=0&clw=256#id=e1b7bc1dfc3f935137e7fb43e0bdd884&currsn=0&ps=56&pc=56
(d)https://www.archiexpo.cn/prod/woodway/product-86598-1832848.html
(e)https://www.renrendoc.com/paper/97249752.htm
(f)https://image.so.com/view?q=HAL%E8%BE%85%E5%8A%A9%E8%A1%8C%E8%B5%B0%E5%9E%8B%E5%BA%B7%E5%A4%8D%E6%9C%BA%E5%99%A8%E4%BA%BA&src=tab_www&correct=HAL%E8%BE%85%E5%8A%A9%E8%A1%8C%E8%B5%B0%E5%9E%8B%E5%BA%B7%E5%A4%8D%E6%9C%BA%E5%99%A8%E4%BA%BA&ancestor=list&cmsid=142efd018611001bf0b38efd12df022f&cmras=6&cn=0&gn=0&kn=0&crn=0&bxn=0&fsn=60&cuben=0&pornn=0&manun=0&adstar=0&clw=256#id=19814fd9c955fc1191cbc7557ad098bb&currsn=0&ps=43&pc=43
2.2. Domestic Lower Limb Exoskeleton Rehabilitation Robots
Compared to international counterparts, research on domestic exoskeleton rehabilitation robots started relatively late in China. However, due to the relentless efforts and continuous innovation of scientists from numerous scientific research institutes and enterprises in our country, many high-performance exoskeleton robots have been developed.
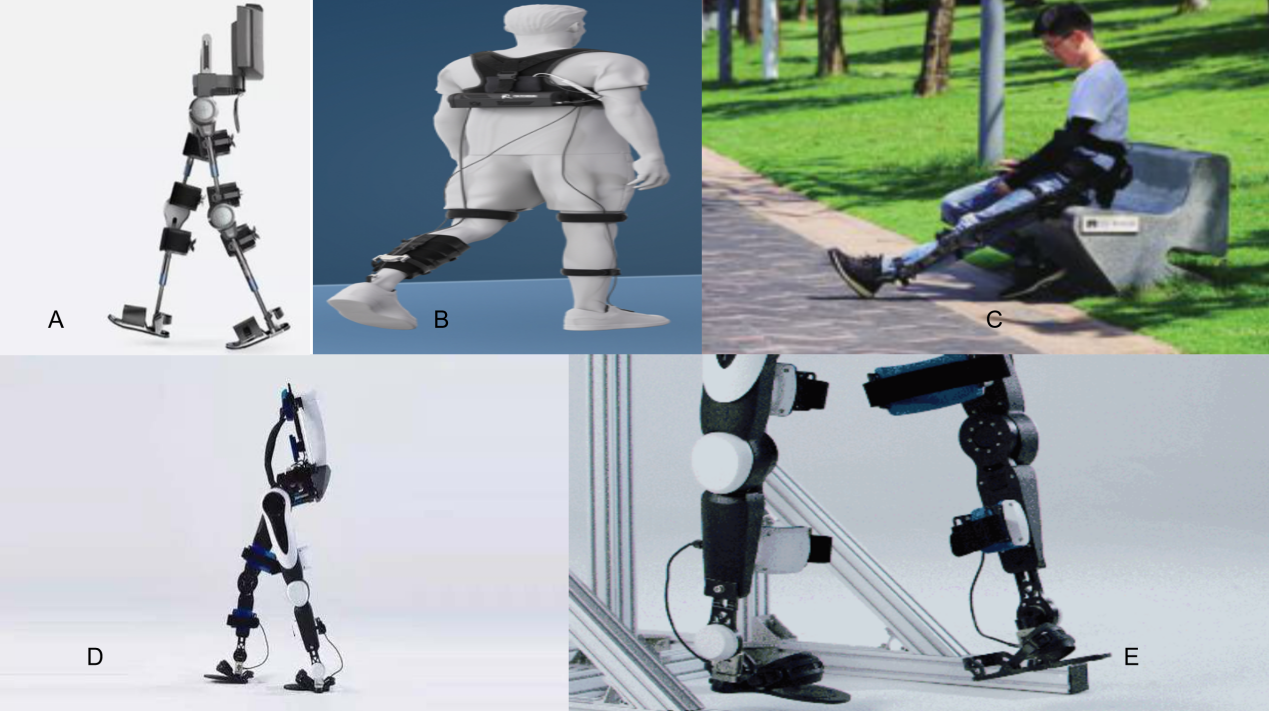
Figure 2. Domestic Lower Limb Exoskeleton Rehabilitation Robots, (a) AiLegs Exoskeleton Robot; (b) Easy Walk X1 Exoskeleton Robot; (c) "Knight" Exoskeleton Robot; (d) Lightweight Flexible Lower Limb Assistive Exoskeleton Robot; (e) Fourier X1 Wearable Lower Limb Exoskeleton Robot.
Picture source:
(a)https://www.xianjichina.com/special/detail 408824.htm
(b)https://www.siyizn.com/zh-cn/product-info.html?id=10037
(c)https://www.doc88.com/p-70459499189150.html
(d)https://image.so.com/view?q=%E5%8F%AF%E7%A9%BF%E6%88%B4%E6%9C%BA%E5%99%A8%E4%BA%BA&src=st&listid=b9a3df24eb3d9c8a574282677ff9fd79&listsrc=wtfsimi&correct=%E5%8F%AF%E7%A9%BF%E6%88%B4%E6%9C%BA%E5%99%A8%E4%BA%BA&ancestor=list&cmsid=8aabf11e6f02b11909f19e6eb6cd11ad&cmras=6&cn=0&gn=0&kn=0&crn=0&bxn=0&fsn=60&cuben=0&pornn=0&manun=0&adstar=0&clw=256#id=b9a3df24eb3d9c8a574282677ff9fd79&currsn=0&ps=68&pc=68
(e)https://zhuanlan.zhihu.com/p/26014960
In 2004, the Hefei Institute of Intelligent Machines, Chinese Academy of Sciences, developed China’s first exoskeleton robot prototype driven by cables, named WPAL [7]. It corrected the human kinematics model, achieving a remarkable milestone by improving the speed-force control model to alleviate muscle fatigue. This initiative marked the inception of exoskeleton robot research in China.
Furthermore, in 2014, Beihang University successfully developed exoskeleton rehabilitation robots such as AiLegs and AiWalker [8]. AiLegs is China’s first exoskeleton rehabilitation robot designed to treat paralysis and hemiplegia. It enables both active and passive forms of rehabilitation training, allowing professional rehabilitation personnel or users themselves to control the robot. The robot can mimic various human walking patterns, driving patients in rehabilitation training, stimulating the neural system, and ultimately achieving the goal of treating paralysis. This design not only significantly improves the efficiency of patient rehabilitation but also provides personalized treatment plans for different diseases, meeting individualized patient needs. DaiAi is a renowned robotics research company in China, and in the field of lower limb exoskeleton robots, AiXing is the new generation of DaiAi’s exoskeleton robot. It provides real-time assistance based on the user’s movement intent, adapting to the user’s capabilities by assessing changes in ground features and surrounding terrain. This helps users activate muscle strength and control gait posture, achieving elegant and natural rapid walking. During the Torch Relay Gathering Ceremony for the Beijing 2022 Winter Paralympics, Shao Haipeng wore the new generation DaiAi AI exoskeleton robot AiXing and successfully completed the torch gathering. With a sensor network and AI control algorithm, it automatically perceives the wearer’s subjective movement intentions, assisting them in moving as desired, switching between fast and slow walking at will, and even performing more complex actions such as climbing stairs and slopes.
Subsequently, in 2018, Shanghai SiYi Intelligent Technology Co., Ltd. developed Easy Walk X1 [9], a novel rehabilitation robot weighing less than 3kg. With no rigid skeleton, it adopts an “electric motor + wire drive” mode, providing assistance to the ankle joints of patients, particularly those suffering from strokes. Additionally, the robot uses artificial intelligence algorithms to identify the timing points requiring assistance during walking, adapting to various walking modes such as flat ground, slopes, and stairs.
In 2019, Shenzhen Kenjin Technology Co., Ltd. introduced a dual-assist lower limb exoskeleton named “Knight”. Unlike Easy Walk X1, this system has both a rigid structure and flexible drive, weighing 5 kg without a battery. It provides active assistance to the hip and knee and is adaptable to different body shapes.
In 2020, Wuhan University of Technology and the Chinese Academy of Sciences jointly developed a lightweight flexible lower limb assistive exoskeleton. Using Bowden ropes and spring devices, the exoskeleton provides assistance to the ankle joint. A single motor at the waist drives both legs, effectively reducing human metabolic rates and making significant contributions to the field of robotics [9].
In 2017, Fourier Intelligent Technology Co., Ltd. in Shanghai developed the wearable lower limb exoskeleton robot Fourier X1 [11]. Unlike similar foreign products, Fourier X1 embodies industrial aesthetics in exoskeleton robots. Engineers at Fourier considered biomechanics and gait from the beginning of the design process, resulting in a lightweight yet fully functional exoskeleton. After numerous design iterations, the final product is an emotionally appealing piece of art.
3. Key Technologies of Lower Limb Exoskeleton Rehabilitation Robots
There is a diverse range of lower limb exoskeleton rehabilitation robots, but the core focus of research on key remains constant. As rehabilitation robot projects advance, the commonalities in technological research become increasingly clear.
3.1. Mechanical Structure Design
The exoskeleton consists of joint-driven components, thigh components, thigh-strapping components, knee joint-driven components, calf components, calf-strapping components, and spring-strapping components. The hip joint-driven component is connected to the thigh component through a connecting plate, and the thigh component has a certain length adjustment range. The design of the knee joint-driven component in the exoskeleton robot fully embodies the principles of bionics and ergonomics, employing a humanoid design approach. This is reflected not only in the specific structural design but also in the realization of the target functions. The structure of the exoskeleton simulates the human lower limbs, especially in the arrangement of each joint and the allocation of degrees of freedom. Human lower limb joints include the hip, knee, and ankle. The hip joint has three degrees of freedom, completing flexion/extension movement around a sagittal axis, abduction/adduction movement around a frontal axis, and external/internal rotation movement around a vertical axis. The knee joint has one degree of freedom for flexion/extension in the sagittal plane, and the ankle joint has three degrees of freedom, including inversion/eversion rotation, dorsiflexion/plantarflexion movement, and slight adduction/abduction movement. Therefore, the unilateral lower limb has seven degrees of freedom. Based on the different joint locations, lower limb exoskeleton robots can be categorized into hip joint rehabilitation exoskeleton robots, knee joint rehabilitation exoskeleton robots, ankle joint rehabilitation exoskeleton robots, and multi-joint combination exoskeleton robots. Exoskeleton robots are characterized by their sturdiness, durability, lightweight, and portability. During use, the mechanical structure must not only bear the weight of various loads carried on the back-mounted shelf but also withstand the impact force from the ground during walking. Therefore, the stiffness of the structure should be ensured first.
The structures of lower limb exoskeleton robots vary widely. The Lokomat is a gait training rehabilitation robot developed by a Swiss company, primarily tasked with physiological gait rehabilitation training. Its main structures include the exoskeleton training system and a medical treadmill. The system mainly comprises a weight reduction system, mechanical legs, and a treadmill. The Lokomat’s unilateral leg includes only two active driven degrees of freedom, allowing movement of the hip and knee joints in the sagittal plane. The Hybrid Assistive Limb (HAL) walking-assist lower limb rehabilitation robot has 26 degrees of freedom, achieving independent support through the combined driving unit of the hip, knee, and ankle joints.
3.2. Drive Systems
The drive system is a prerequisite in the design of robot structures and control, enhancing the feasibility and convenience of the robot’s operation. For instance, the Lokomat lower limb exoskeleton robot developed by the Swiss company Hocoma and the wearable lower limb exoskeleton robot KCL developed by Tsukuba University in Japan both feature drive systems with characteristics such as high transmission efficiency, lightweight, small volume, and low energy consumption. More importantly, the drive systems exhibit quick operational response, enabling prompt analysis of patient movements and driving the robot to react accordingly. Common drive methods for lower limb exoskeleton robots include hydraulic drive, pneumatic drive, and electric motor drive. Hydraulic and pneumatic drives share similar principles, exerting relatively low forces, making them suitable for patients actively engaging in rehabilitation training. In comparison, electric motor drive offers accurate and efficient performance, making it suitable for patients undergoing passive rehabilitation training. Electric motors boast high drive precision, ease of automation control, and fast operational response, rendering them the prevailing drive method for lower limb exoskeleton robots. However, due to the momentary high power output of electric motor drive, it requires a carefully designed software control program to ensure a suitable match during the design process.
3.3. Robot Control Methods
The control system, as a critical component governing the operation of robot programs, plays a pivotal role in the functionality and utilization of the robot. Initially, through the perceptual function of the exoskeleton robot and the sensor structure within the robot, it acquires the motion intent of physiological activities performed by the patient. Based on the analysis and processing of this information, it executes the optimal rehabilitation training plan. The entire process demands a fundamental capability for rapid and precise information processing speed. This is an essential functionality that lower limb exoskeleton rehabilitation robots must possess.
3.4. Human-Machine Interaction
Human-machine interaction refers to the coordination between patients and robots and the efficiency of patient rehabilitation. In the research of exoskeleton lower limb rehabilitation robots, various training modes exist, primarily including active training mode, assistance training mode, impedance training mode, and passive training mode, corresponding to the rehabilitation of patients’ knee and hip joints. Patients complete rehabilitation training with the assistance of the robot. Under the purely active training mode, the rehabilitation effect for patients is not significant. This is fundamentally because stroke patients have not established a deep neural structure in the cerebral cortex, making it challenging for them to detach from the exoskeleton rehabilitation robot. Therefore, to better aid patients in treating brain damage, it is essential to enhance patients’ brain control over their limbs. Simultaneously, patients should actively complete rehabilitation training with the assistance of the exoskeleton rehabilitation robot to achieve the desired effects in treating strokes.
3.5. Methods Based on Physiological Electrical Signals
In traditional robot control algorithms, the commonly employed method for precise control of robot positions is force-position hybrid control. However, with clinical experiments demonstrating its relatively low efficiency, an alternative control method, based on electrical signals, has emerged. Under the influence of electrical signals, the robot’s control algorithm becomes more accurate and efficient, capable of making adjustments and adaptations in real-time according to the patient’s physiological movements. In comparison to force-position hybrid control, this electrical signal control method poses less harm to patients, making it the preferred control method for many contemporary lower limb exoskeleton rehabilitation robots.
4. Rehabilitation Training Prescription
4.1. Movement Function Assessment
Traditional methods for assessing movement function often rely on scales or records kept by rehabilitation physicians, which can carry a degree of subjectivity. Nowadays, we gauge the extent of patients’ recovery in rehabilitation training through the data recorded by exoskeleton rehabilitation robots. Specifically, we use computer-generated data to adjust the intensity of rehabilitation training, aiming to meet the personalized needs of patients and clearly identify the stage of their rehabilitation, thereby enhancing treatment efficiency. Throughout the patient’s recovery process, we statistically analyze the robot’s gait position and speed information during training, visually representing the therapeutic effects through data comparison.
By adjusting the magnitude of the assistive force provided during training, we encourage patients to actively engage in rehabilitation exercises. This approach involves the repetitive execution of rehabilitation training actions with greater accuracy, utilizing pre-designed programs for a more precise rehabilitation process.
4.2. Rehabilitation Robot Training Modes
The rehabilitation methods of exoskeleton rehabilitation robots can be categorized into three types: passive rehabilitation, assistive rehabilitation, and active rehabilitation. These training modes primarily include passive training, assistive training, active training, and impedance training. Passive training relies entirely on the exoskeleton robot to provide the driving force to move the human body and is generally applied in the early stages of patient rehabilitation. When the patient’s lower limb has insufficient active force, the exoskeleton robot provides assistance to facilitate training. In the mid-to-late stages of rehabilitation, patients often adopt the active training mode. At this point, patients have regained a certain level of muscle strength, leading the rehabilitation process themselves, with the exoskeleton robot serving as an auxiliary device to assist in complex gait rehabilitation training. Impedance training mode is applied in the later stages of rehabilitation when the primary goal is to enhance muscle strength. The robot provides resistance for rehabilitation training. Due to individual differences among patients, it is necessary to selectively choose training modes at different stages of rehabilitation to gradually restore physical functions.
5. Conclusion
With the advancement of science and technology, the development and application research of lower limb rehabilitation robots have become increasingly widespread, signifying the significant importance of exoskeleton robots in the field of rehabilitation. The key technologies for exoskeleton robots primarily involve the design of mechanical structures, control algorithms, human-machine interaction techniques, and driving modes. In the research process in China, efforts have been made to narrow the gap between clinical medicine and lower limb robotic technology. Presently, there is a need to explore, stimulate, and manipulate the neuroplasticity mechanisms of the brain as much as possible. In terms of clinical application, corresponding lower limb robots should be subjected to large-scale clinical trials among patients with lower limb motor dysfunction caused by neurological diseases such as stroke. Carefully designed clinical studies should demonstrate the advantages of exoskeleton robots in gait rehabilitation, providing high-intensity and highly repetitive motion training. This significantly reduces the burden on medical institution staff. Future research should clearly define the effective characteristics and methods of robot-assisted therapy, determining the trajectories and sensory inputs that robots must provide to enhance the quality and efficiency of patient rehabilitation.
References
[1]. Milia P de Salvo F, Caserio M, et al. Neurorehabilitation inparaplegic patients with an active powered exoskeleton (Ekso)J].Digital Medicine, 2016, 2(4): 163-168.
[2]. Technaid. Technaid at Global Robot Expo 2019EB/OL].(2018-05-11) [2022-03-28].
[3]. Xu, F., Lu, G. N., Cheng, Y. Z., et al. (2018). Advances in Structural Design of Lower Limb Rehabilitation Robots. Beijing Biomedical Engineering, 2018, 37(1), 96-102.
[4]. Ding, Y. W., Tu, L. J., Liu, Y. X., Zhang, J. C., & Shuai, M. (Beijing University of Aeronautics and Astronautics, Beijing 100191). Advances in Research on Wearable Lower Limb Exoskeleton Rehabilitation Robots.
[5]. Farris R J, Quintero H A, Goldfarb M. Preliminary evaluationof a powered lower limb orthosis to aid walking in paraplegiindividuals[J]. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2011,19(6): 652-659.
[6]. Zhang, F., Yu, H. L., Wang, L. L., et al. (2017). Discussion on Classification of Rehabilitation Robots. Chinese Journal of Physical Medicine and Rehabilitation, 2017, 39(8), 633-636.
[7]. Fang, Y. (2009). Dynamics Modeling and Control Research on Wearable Lower Limb Assistive Robots [Doctoral dissertation, University of Science and Technology of China].
[8]. Beijing DaAi Robot Technology Co., Ltd. AiLegs Product Introduction [EBOL]. [Retrieved on March 28, 2022].
[9]. Zhao, X. G., Tan, X. W., Zhang, Q. (2020). Research Progress and Key Technology Analysis of Flexible Lower Limb Exoskeleton Robots. Robotics, 2020, 42(3), 365-384.
[10]. Zhao, X. G., Tan, X. W., Zhang, Z. (2020). Research Progress and Key Technology Analysis of Flexible Lower Limb Exoskeleton Robots. Robotics, 2020, 42(3), 365-384.
[11]. Shanghai Fourier Intelligent Technology Co., Ltd. Fourier X2 Product Introduction [EB/L]. [Retrieved on July 21, 2019].
Cite this article
Liu,H. (2024). Current status and future trends in lower limb exoskeleton rehabilitation robots. Applied and Computational Engineering,65,153-160.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of Urban Intelligence: Machine Learning in Smart City Solutions - CONFSEML 2024
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Milia P de Salvo F, Caserio M, et al. Neurorehabilitation inparaplegic patients with an active powered exoskeleton (Ekso)J].Digital Medicine, 2016, 2(4): 163-168.
[2]. Technaid. Technaid at Global Robot Expo 2019EB/OL].(2018-05-11) [2022-03-28].
[3]. Xu, F., Lu, G. N., Cheng, Y. Z., et al. (2018). Advances in Structural Design of Lower Limb Rehabilitation Robots. Beijing Biomedical Engineering, 2018, 37(1), 96-102.
[4]. Ding, Y. W., Tu, L. J., Liu, Y. X., Zhang, J. C., & Shuai, M. (Beijing University of Aeronautics and Astronautics, Beijing 100191). Advances in Research on Wearable Lower Limb Exoskeleton Rehabilitation Robots.
[5]. Farris R J, Quintero H A, Goldfarb M. Preliminary evaluationof a powered lower limb orthosis to aid walking in paraplegiindividuals[J]. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 2011,19(6): 652-659.
[6]. Zhang, F., Yu, H. L., Wang, L. L., et al. (2017). Discussion on Classification of Rehabilitation Robots. Chinese Journal of Physical Medicine and Rehabilitation, 2017, 39(8), 633-636.
[7]. Fang, Y. (2009). Dynamics Modeling and Control Research on Wearable Lower Limb Assistive Robots [Doctoral dissertation, University of Science and Technology of China].
[8]. Beijing DaAi Robot Technology Co., Ltd. AiLegs Product Introduction [EBOL]. [Retrieved on March 28, 2022].
[9]. Zhao, X. G., Tan, X. W., Zhang, Q. (2020). Research Progress and Key Technology Analysis of Flexible Lower Limb Exoskeleton Robots. Robotics, 2020, 42(3), 365-384.
[10]. Zhao, X. G., Tan, X. W., Zhang, Z. (2020). Research Progress and Key Technology Analysis of Flexible Lower Limb Exoskeleton Robots. Robotics, 2020, 42(3), 365-384.
[11]. Shanghai Fourier Intelligent Technology Co., Ltd. Fourier X2 Product Introduction [EB/L]. [Retrieved on July 21, 2019].