






1. Introduction
As humans enter the crisis drama of an aging society, the vast majority of people begin to show serious tendencies such as dementia, epilepsy, and brain atrophy between the ages of 50 and 70. The challenges that older people encounter include not just the deterioration of mental functions like memory and cognition, but also the diseases that have led to a precipitous reduction in their quality of life. Brain-computer interfaces, as a promising and increasingly popular technology, are being incorporated into the treatment of many patients with cognitive or physical disorders. These interfaces bypass the need for conventional neuromuscular channels and enable direct contact between the brain and external equipment. Patients suffering from conditions like Parkinson's disease (PD) and Alzheimer's disease (AD) benefit greatly from this technology since it gives them new opportunities to engage with the community and prolong their independence.
The field of brain-computer interface (BCI) study can date back to the late 1800s, when investigations conducted by Richard Caton revealed that the animal brain exhibited continuous electrical activity. This discovery laid the foundation for the future development of neuroscience technology [1]. By the 1990s, BCI technology began to be tested in clinical settings, and after 2000, research and application accelerated further with Jonathan Wolpaw's definition of BCI technology [2].
The core function of the BCI system is to record neural signals from the brain, process the signals through computer algorithms, and use external devices to convert the processed signals into expected actions. The signals captured by brain-computer interfaces (BCI) originate from ongoing electrophysiological, neurochemical, and metabolic activities in the central nervous system, including neuronal action potentials, synaptic potentials, and neurotransmitter release. The basic structure of BCI as shown in the Figure 1 includes signal acquisition, preprocessing, signal translation and external device control [3].
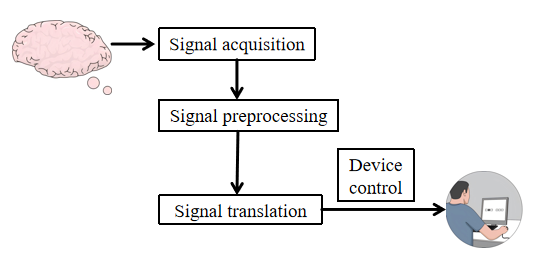
Figure 1. The structure of brain computer interface (Figure Credits: Original).
The mechanism of action of BCI is mainly to stimulate neuroplasticity through neurofeedback training. Neuroplasticity refers to the property of neurons to undergo adaptive changes to maintain stability after being stimulated by external factors, and is an important basis for the rehabilitation of neurological diseases. Neuroplastic changes are mainly manifested in neurogenesis, changes in neuronal excitability and transmission, and changes in synaptic connections between neurons. Neurofeedback training is to record the neural signals of the patient's brain through BCI, analyze the patient's intentions, issue action instructions, and then provide visual, auditory, tactile and other feedback based on the completion of the instructions, forming a closed-loop control pathway to unify the action intention and behavior. Repeated stimulation will be produced during the training process, including paired stimulation and closed-loop stimulation on the neural pathway, thereby promoting the activation of related cortical neurons, such as visually guided feedback movement training, which can effectively activate the brain's sensory motor cortex during the learning process [4].
BCI has a wide range of applications in the medical field, especially in dealing with neurodegenerative diseases such as AD and PD. A major application area of BCI technology is neurorehabilitation, where these technologies are used to help patients recover functions lost due to disease or injury. For example, BCI technology can be used to restore motor function, enhance mobility and improve communication, and can also restore hearing and vision through neuroprosthetic devices [1]. BCI also shows great potential in improving diagnostic accuracy and neurorehabilitation. In particular, for patients with impaired consciousness, traditional behavioral assessment methods are often difficult to accurately diagnose, while BCI can provide more accurate diagnosis by combining Electroencephalograph (EEG) and visual tasks to detect the patient's covert response level [1].
AD and PD are major neurodegenerative conditions that significantly affect the elderly. AD is known for its progressive decline in cognitive functions, while PD primarily affects motor abilities, causing symptoms like bradykinesia, stiffness, and tremors. Currently, approximately 24 million people globally suffer from AD, with projections suggesting that this number could double by 2050. PD stands as the second most prevalent neurological condition, impacting 1.7% of individuals over 65 and increasing to 10% among those over 80. These statistics and the graphs below underline the substantial burden these diseases place on the aging population, highlighting the urgent need for effective medical and social interventions. Figure 2 and Figure 3 demonstrate the global trend of AD and PD in 2021. Since this article is more concerned with BCI-based applications, for readers interested in clinical symptoms, this work recommends obtaining more information related to clinical symptoms from other sources [5].
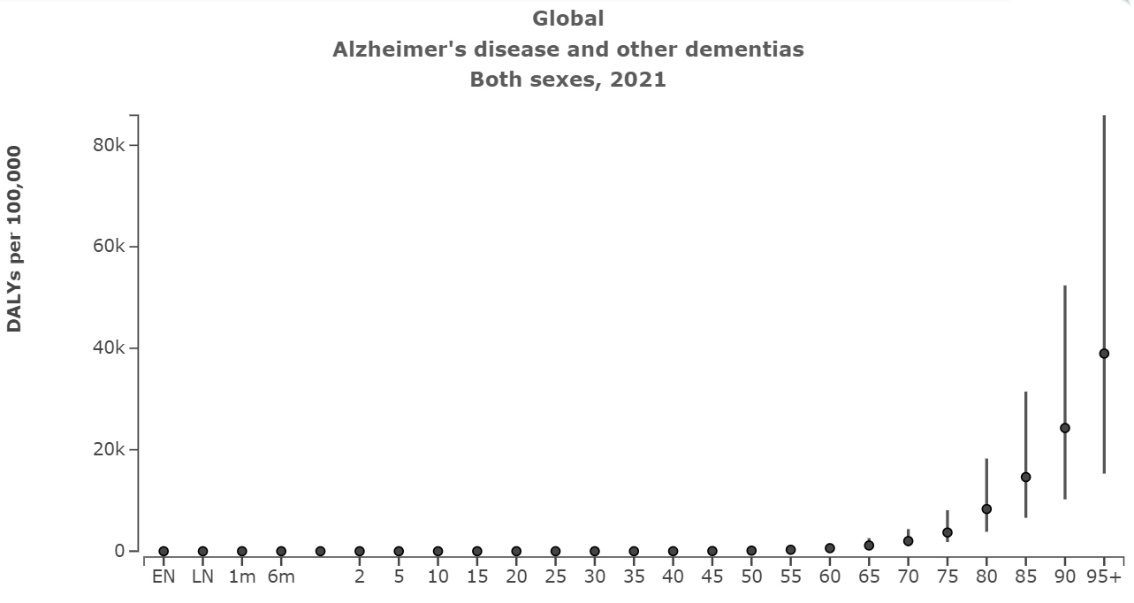
Figure 2. Global distribution of Disability-Adjusted Life Years (DALYs) for Alzheimer’s Disease segmented by age in 2021 [6].
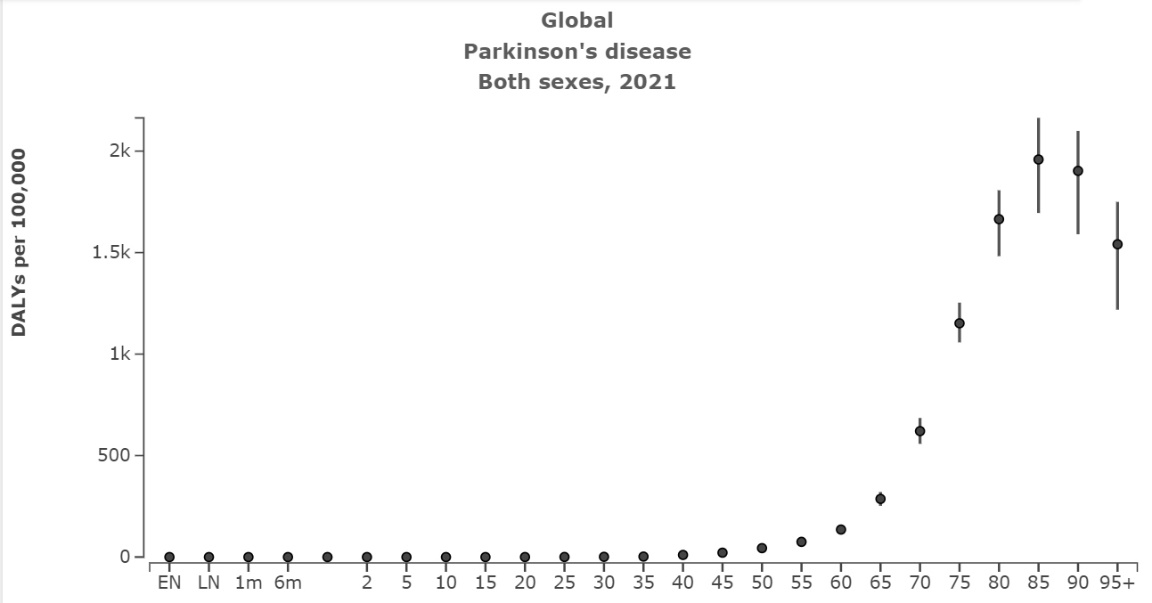
Figure 3. Global distribution of Disability-Adjusted Life Years (DALYs) for Parkinson's Disease segmented by age in 2021 [6].
2. BCI-based cognitive enhancement in Alzheimer’s disease
Recent advancements in BCI technology have opened new avenues for cognitive enhancement and memory improvement. Taya et al. explored the potential of BCI-based cognitive training, demonstrating significant improvements in memory and cognitive function over an 8-week training period with 50 participants [7]. Oh and Ryu conducted a study to explore the impact of BCI cognitive training on individuals suffering from dementia., finding notable cognitive improvements in a randomized control trial involving 30 participants [8]. Carelli et al. provided a comprehensive review of BCI applications for rehabilitation and cognitive evaluation, highlighting the benefits of EEG-based BCIs for patients with neurological conditions [9]. These studies collectively underscore the effectiveness of BCI technology in enhancing cognitive functions and provide a robust foundation for further research in this domain.
In 2015, Taya et al. conducted a study to explore the potential of BCI in assisting cognitive rehabilitation for enhancing memory and cognitive function [7]. They designed an experimental method involving a BCI system that provided real-time feedback to participants engaged in various cognitive tasks. The study involved a sample size of 50 participants who underwent cognitive training sessions over a period of 8 weeks. The data collected included pre- and post-training cognitive assessments using standardized tests. The results demonstrated significant improvements in participants' memory and cognitive function, supporting the conclusion that this training is a viable technique for cognitive enhancement.
In 2018, researchers Se-Jung Oh and Jeon-Nam Ryu conducted an experimental research on the impact of BCI-based cognitive training for elderly patients with dementia. Thirty patients were involved in the research study, with treatment and control groups being selected at random. A brain-computer interface was used in the treatment group's cognitive training sessions to enhance cognitive capacities through gaming components. Meanwhile, the control group engaged in activities like gymnastic exercises and music listening. Over the course of six weeks, participants completed eighteen forty-minute sessions. Cognitive function was assessed using the Korean Dementia Rating Scale (K-DRS) and the Mini-Mental State Examination-Korean (MMSE-K). The results revealed significant cognitive gains in the treatment group, highlighting the potential of BCI-based cognitive exercises as a beneficial approach for enhancing mental functions in patients with dementia.
Laura Carelli et al. provided a comprehensive overview of BCI applications for cognitive assessment and rehabilitation [9]. They examined various studies employing BCI technology for patients with neurological conditions. The authors highlighted the use of EEG-based BCIs to develop cognitive assessment tools and neurofeedback systems for cognitive training. They discussed the benefits of BCIs in providing real-time feedback, enhancing patient motivation, and improving neural plasticity. The review covered a broad range of studies, involving thousands of participants, and concluded that BCI-based cognitive training holds promise for both clinical assessment and rehabilitation, offering a novel approach to enhancing cognitive functions in patients with severe motor and cognitive impairments.
Recent studies have introduced innovative approaches leveraging advanced technologies to enhance cognitive functions. One promising direction involves the integration of extended reality (XR) and BCI technology [10]. This approach focuses on developing immersive cognitive training systems that utilize mixed reality (MR) and virtual reality (VR) environments combined with real-time brainwave monitoring to enhance cognitive responses and sensory perception. By detecting and analyzing neural activity through EEG sensors, these systems provide real-time feedback during multifaceted cognitive tasks, such as the Stroop Effect, Schulte Grid, Eureka Effect, and Soma Cube exercises. These tasks are designed to improve various cognitive functions, including logical thinking, memory, spatial awareness, and problem-solving abilities.
The innovative use of XR and BCI technology allows for personalized and adaptive cognitive training, where the difficulty of tasks can be adjusted based on real-time brainwave data, ensuring that the training remains challenging and effective. Additionally, the incorporation of telemedicine capabilities via platforms like Microsoft Mesh and HoloLens 2 expands the reach of cognitive training, making it accessible to remote users and facilitating collaborative medical education and rehabilitation. This integration not only enhances the effectiveness of cognitive training but also provides a scalable solution for addressing cognitive impairments in diverse populations.
3. BCI applications in Parkinson’s disease
3.1. BCI-based therapy in tremor control
Parkinson's disease is recognized as a prevalent neurodegenerative disorder, distinguished by its signature symptoms including tremors, muscle stiffness, slowness of movement, and impaired balance. Progress has been made in the management of this debilitating disease through the application of BCI and drug therapies. The standard treatment regimen for Parkinson's includes medications like levodopa and amantadine. However, when these drugs are not effective or yield fluctuating results, it is crucial to consider alternative treatment options. One such alternative is deep brain stimulation (DBS).
In 2023, a study examined how a new 32-contact directional DBS electrode impacts the neuronal network dynamics in Parkinson's disease [11]. They focused on stimulating the subthalamic nucleus (STN) and compared the results with those of conventional DBS. Utilizing a computational model composed of 1280 conductance-based Hodgkin-Huxley neurons, they explored five different stimulation patterns: anterior, posterior, lateral, medial, and spherical. The study revealed that directional DBS significantly enhanced thalamic relay performance and reduced pathological neuronal oscillations more effectively than spherical DBS. The researchers concluded that directional DBS provides a wider therapeutic window and better management of pathological neural activity, making it a promising approach for treating Parkinson's disease.
In 2010, Grimaldi and Manto explored various therapies for managing human tremor, focusing on both established and new treatments [12]. The review detailed the significant role of DBS in treating tremors, particularly those that are resistant to medicine in diseases such as PD and essential tremor. They compared the efficacy and safety of DBS with traditional surgical methods like thalamotomy and pallidotomy. Additionally, the review discussed innovative approaches in bioengineering, such as functional electrical stimulation (FES) and BCIs, which show potential in managing tremor symptoms. The authors concluded that integrating these novel methods with traditional treatments could improve therapeutic outcomes for patients.
In 2022, Ferrazoli and his team investigated the use of P300-long-latency auditory-evoked potentials (P300-LLAEP) to assess cognitive function in Parkinson's patients undergoing DBS [13]. The study, conducted with 45 patients receiving bilateral subthalamic nucleus DBS, involved collecting cognitive function data before and after surgery using P300-LLAEP measurements. The results indicated that P300-LLAEP effectively reflected changes in cognitive function post-DBS. According to the investigation result, for PD patients treated with DBS, incorporating P300-LLAEP into clinical evaluations is an excellent way to enhance the monitoring and control of cognitive outcomes
3.2. BCI-based motor imagery in tremor control
For several years, researchers have dedicated efforts to investigating how BCI technology can be utilized in managing and treating symptoms linked to PD. Various strategies have been assessed to enhance motor skills and overall standard of life for individuals with PD, ranging from improved motor imagery BCIs to pharmaceutical therapies.
In 2017, Jeffrey V. Rosenfeld and Yan Tat Wong conducted a review to explore the advancements and future potential of neurobionics and BCIs in various applications, including motor imagery for movement disorders [14]. The review concentrated on the fusion of electronics with the nervous system to support individuals who are paralyzed and those suffering from movement disorders like Parkinson's disease. It explained that BCIs interpret electrical signals from the motor cortex to manage robotic limbs and exoskeletons, enhancing motor skills and agility. While these technologies are still in their initial stages, they have demonstrated encouraging outcomes in facilitating movement and enhancing life quality for people with significant motor disabilities. The authors emphasized that more technical advancements and extensive clinical studies are needed before these applications can be broadly implemented in clinical settings.
In 2020, Shi and colleagues conducted research to improve the accuracy of motor imagery-based BCIs by enhancing feature extraction methods for EEG signals [15]. The research included 30 participants who engaged in motor imagery exercises while their EEG signals were monitored. The scientists introduced a novel method for extracting features, utilizing common spatial pattern (CSP) and wavelet packet decomposition (WPD), aimed at improving the classification of motor imagery signals. The experimental methodologies included a comparative analysis with traditional feature extraction methods. Results demonstrated that the proposed technique significantly improved classification accuracy, supporting its potential application in motor imagery-based BCI systems for assisting Parkinson's patients. The authors came to the conclusion that their technique offers a viable way to improve the dependability and efficiency of BCI applications.
Ren et al. looked at the rehabilitation of Parkinson's patients using an improved motor imagery-based BCI [16]. Conducted at a rehabilitation center, the study included 25 patients with Parkinson's disease who participated in BCI training sessions over 12 weeks. The experimental method involved using a combination of motor imagery tasks and real-time feedback to improve motor function. Data collected included pre- and post-intervention assessments of motor skills and EEG signal analysis. The results showed significant improvements in motor function and neural activity patterns, suggesting that enhanced motor imagery-based BCIs can be an effective tool for rehabilitation in Parkinson's patients. The study concluded that incorporating advanced signal processing techniques and real-time feedback can optimize the therapeutic outcomes of BCI interventions.
4. Communication aids for both AD and PD
Communication barriers significantly impact the standard of life for individuals with AD and PD, leading to increased isolation and decreased independence. BCIs are now recognized as a viable tool for addressing these issues by offering alternative communication pathways that bypass traditional motor and cognitive capabilities. BCIs utilize neural signals to facilitate direct interaction with computers and other digital devices, enabling patients to communicate more effectively despite their impairments.
BCIs have been empirically demonstrated in recent studies to improve communication in individuals with PD and AD. For instance, studies like those by Chen et al. have developed high-speed spelling systems using non-invasive EEG-based BCIs, allowing users to communicate through character selection with impressive speed and accuracy [17]. Ebrahimi et al. explored the use of BCIs in multimedia communication, showing that EEG signals can manage multimedia environments, thus creating new avenues of communication for individuals with significant motor limitations [18]. Additionally, Lazarou et al. evaluated EEG-based BCIs for improving communication in patients with communication impairments, highlighting significant improvements in accuracy and efficiency [19]. These improvements in BCI technology mark a major advance in overcoming communication challenges faced by individuals with AD and PD, enabling them to articulate their needs and thoughts more effectively. The ongoing enhancement and refinement of BCI systems offer great potential for bettering conversational skills and overall life quality for those affected by these profound conditions.
In 2015, Chen and colleagues conducted a study to develop a high-speed, non-invasive BCI for spelling [17]. They designed a system using EEG to detect user intentions and translate them into text at high speed. The study involved 12 participants who used the BCI system in a series of sessions to spell words by selecting characters from a visual matrix. The researchers validated their system using performance metrics such as speed and accuracy of character selection. Data collected included EEG signals and spelling accuracy rates. The results showed that participants could achieve high spelling speeds with satisfactory accuracy. The study concluded that the proposed BCI system is effective for communication enhancement, offering a fast and reliable means of non-verbal communication for individuals with motor impairments.
In 2003, Touradj Ebrahimi, etc. investigated the potential of BCIs in enhancing multimedia communication [18]. Their research aimed to create BCI systems that would enable users to engage with multimedia information via brain signals. They concentrated on EEG-based BCIs and experimented with several signal processing approaches to improve their accuracy and efficiency. The study involved experiments with multiple participants, where EEG signals were recorded and analyzed to control multimedia applications. The researchers collected extensive EEG data and utilized advanced signal processing algorithms to interpret user intentions. The results demonstrated that BCIs could effectively be used for multimedia control, providing a novel communication channel for users with severe motor disabilities. The study concluded that BCIs have significant potential in multimedia communication, requiring further development to enhance their usability and reliability.
In 2018, Lazarou etc. conducted a study to evaluate the effectiveness of EEG-based BCIs for communication enhancement in patients with communication impairments [19]. The research involved 20 participants with varying degrees of motor and communication disabilities. The experimental method included using an EEG-based BCI system to promote communication through a computer interface. Participants underwent multiple sessions where they were trained to use the BCI for selecting words and phrases. Data collected included EEG signals, selection accuracy, and communication speed. The study found that participants showed significant improvements in communication abilities, with increased accuracy and reduced time required to convey messages. The researchers concluded that EEG-based BCIs are a viable tool for enhancing communication in individuals with severe disabilities, highlighting the need for personalized training and adaptive algorithms to improve performance further.
5. Discussion
5.1. Limitations of BCI
DBS is a recognized treatment for PD, but it comes with several limitations and potential side effects. One significant limitation is the variability in patient response to the treatment. While DBS can alleviate motor symptoms and reduce the need for medications like levodopa, it does not equally benefit all patients and can even exacerbate certain conditions such as speech and cognitive functions. Specifically, patients undergoing STN stimulation might experience a decline in verbal fluency and cognitive abilities compared to those receiving Globus Pallidus internus (GPi) stimulation, which tends to have fewer cognitive side effects but may not reduce medication needs as effectively [20].
Moreover, DBS can lead to the development of dyskinesias, which are involuntary, erratic movements that can be as debilitating as the original PD symptoms. Dyskinesias may result from both levodopa treatment and DBS itself, particularly if the stimulation parameters are not optimally adjusted in real time. Another critical issue is the "brittle response" seen in some patients, where they fluctuate between states of bradykinesia and dyskinesia with minimal periods of optimal motor function. These patients, often younger females with early disease onset, experience severe side effects that are challenging to manage with current DBS protocols [4].
Efforts to mitigate these side effects include developing closed-loop DBS (CLDBS) systems that adjust stimulation parameters based on real-time neural feedback. Such systems aim to reduce unnecessary stimulation and associated side effects by tailoring the treatment to the patient's current state. To guarantee their effectiveness and safety, these systems still need to undergo additional validation as they remain in the experimental stage.
5.2. Ethical concerns of BCI
The ethical landscape of Brain-Computer Interfaces (BCIs) is complex, encompassing critical concerns regarding data confidentiality and integrity, physiological and psychological harms, mental autonomy, and equitable access to technology. Privacy issues arise from potential data breaches, cryptographic attacks, and unauthorized use of neural data, necessitating robust measures such as encryption, data anonymization, and stringent access controls to safeguard user information [21]. Additionally, ensuring mental autonomy is paramount, particularly as BCIs evolve to interpret complex neural signals, which could inadvertently influence user thoughts and behaviors. Equitable access to BCI technology remains a significant ethical issue, with current high costs potentially exacerbating socioeconomic disparities. Effective ethical practices involve the integration of ethics expertise through embedded ethicists within research teams, fostering continuous, bidirectional ethical input and mutual learning [21]. This collaborative approach promotes shared responsibilities and spontaneous ethical discussions, guaranteeing that ethical issues are addressed organically during the research process.
5.3. Future directions
Future research in BCIs holds promising potential for aiding Parkinson's and Alzheimer's patients beyond communication and cognitive enhancements. One significant area is the development of BCI-controlled assistive devices, such as wheelchairs and exoskeletons, which can improve mobility and independence for Parkinson's patients suffering from severe motor impairments [22]. Additionally, BCIs can facilitate neurorehabilitation by leveraging real-time neural feedback to enhance motor function and assist in physical therapy regimens, potentially aiding in the recovery of motor skills [23]. For Alzheimer's patients, BCIs could be employed in monitoring and managing cognitive decline by providing early detection of neural degradation and enabling interventions to slow down the progression of the disease [24]. Furthermore, the application of artificial intelligence in BCIs, such as machine learning algorithms for signal processing and pattern recognition, can significantly improve the accuracy and efficiency of these systems, providing more personalized and adaptive interventions for patients [23].
6. Conclusion
The integration of BCI technology into the management and treatment of Alzheimer's and Parkinson's diseases represents a pivotal advancement in neurorehabilitation. By enabling novel pathways for cognitive enhancement, motor function restoration, and communication, BCIs provide essential tools for improving the independence and standard of life of affected individuals. From the inception of BCI in early EEG experiments to today’s sophisticated applications in neurofeedback, the evolution of this technology underscores its significant potential in healthcare. While challenges like ensuring signal accuracy and maintaining ethical standards remain, ongoing research and technological advancements are poised to overcome these barriers. Future directions point towards developing BCI-controlled assistive devices and integrating artificial intelligence to tailor more effective and personalized interventions, highlighting the transformative impact of BCIs in treating neurodegenerative disorders.
References
[1]. Young, M. J., Lin, D. J., & Hochberg, L. R. (2021). Brain–Computer interfaces in neurorecovery and neurorehabilitation. In Seminars in neurology, 41(02), 206-216.
[2]. Wolpaw, J. R., Millan, J. D. R., & Ramsey, N. F. (2020). Brain-computer interfaces: Definitions and principles. Handbook of clinical neurology, 168, 15-23.
[3]. Mudgal, S. K., Sharma, S. K., Chaturvedi, J., & Sharma, A. (2020). Brain computer interface advancement in neurosciences: Applications and issues. Interdisciplinary Neurosurgery, 20, 100694.
[4]. Jackson, A., & Zimmermann, J. B. (2012). Neural interfaces for the brain and spinal cord—restoring motor function. Nature Reviews Neurology, 8(12), 690-699.
[5]. Alzheimer’s Disease Fact Sheet, National Institute on Aging. URL: https://www.nia.nih.gov/health/alzheimers-and-dementia/alzheimers-disease-fact-sheet. Last Accessed: 2024/08/04.
[6]. GBD Compare, Institute for Health Metrics and Evaluation. URL: http://vizhub.healthdata.org/gbd-compare. Last Accessed: 2024/08/04.
[7]. Taya, F., Sun, Y., Babiloni, F., Thakor, N., & Bezerianos, A. (2015). Brain enhancement through cognitive training: a new insight from brain connectome. Frontiers in systems neuroscience, 9, 44-63.
[8]. Oh, S. J., & Ryu, J. N. (2018). The effect of brain-computer interface-based cognitive training in patients with dementia. Journal of the Korean Society of Physical Medicine, 13(4), 59-65.
[9]. Carelli, L., Solca, F., Faini, A., Meriggi, P., et, al. (2017). Brain‐computer interface for clinical purposes: Cognitive assessment and rehabilitation. BioMed research international, 2017(1), 1695290.
[10]. Lin, P. J., Ku, H. C., & Lin, L. L. (2024). Design and Development of Cognitive Training Systems Based on Extended Reality and BCI Technology. In 2024 IEEE 7th Eurasian Conference on Educational Innovation, 4-7.
[11]. Denggui, F., Suyu, L., Zhihui, W., Qingyun. W., (2015). The control effect of deep brain stimulation on the dynamics of neuronal networks in Parkinson's disease (Chinese). In Proceedings of the 15th National Conference on Nonlinear Vibration and the 12th National Conference on Nonlinear Dynamics and Stability of Motion, 1.
[12]. Grimaldi, G., & Manto, M. (2010). Old and emerging therapies of human tremor. Clinical Medicine Insights: Therapeutics, 2, 2999.
[13]. Ferrazoli, N., Donadon, C., Rezende, A., Skarzynski, P. H., & Sanfins, M. D. (2022). The application of P300-long-latency auditory-evoked potential in Parkinson disease. International archives of otorhinolaryngology, 26(01), 158-166.
[14]. Rosenfeld, J. V., & Wong, Y. T. (2017). Neurobionics and the brain–computer interface: current applications and future horizons. Medical Journal of Australia, 206(8), 363-368.
[15]. Shi, T., Ren, L., & Cui, W. (2019). Feature extraction of brain–computer interface electroencephalogram based on motor imagery. IEEE Sensors Journal, 20(20), 11787-11794.
[16]. Ren, S., Wang, W., Hou, Z. G., Liang, X., Wang, J., & Shi, W. (2020). Enhanced motor imagery based brain-computer interface via FES and VR for lower limbs. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 28(8), 1846-1855.
[17]. Chen, X., Wang, Y., Nakanishi, M., Gao, X., Jung, T. P., & Gao, S. (2015). High-speed spelling with a noninvasive brain–computer interface. Proceedings of the national academy of sciences, 112(44), E6058-E6067.
[18]. Ebrahimi, T., Vesin, J. M., & Garcia, G. (2003). Brain-computer interface in multimedia communication. IEEE signal processing magazine, 20(1), 14-24.
[19]. Lazarou, I., Nikolopoulos, S., Petrantonakis, P. C., Kompatsiaris, I., & Tsolaki, M. (2018). EEG-based brain–computer interfaces for communication and rehabilitation of people with motor impairment: a novel approach of the 21st Century. Frontiers in human neuroscience, 12, 14.
[20]. Benabid, A. L. (2003). Deep brain stimulation for Parkinson’s disease. Current opinion in neurobiology, 13(6), 696-706.
[21]. Yue, C. (2023). Privacy and Ethical Concerns of Brain-Computer Interfaces. In 2023 IEEE International Conference on Metaverse Computing, Networking and Applications, 134-138.
[22]. Limchesing, T., Chua, A., Shi, C., Baldovino, R., et, al. (2021). A review on recent applications of EEG-based BCI in wheelchairs and other assistive devices. In 2021 IEEE 13th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment, and Management, 1-6.
[23]. Karikari, E., & Koshechkin, K. A. (2023). Review on brain-computer interface technologies in healthcare. Biophysical Reviews, 15(5), 1351-1358.
[24]. Patel, N., Verma, J., & Jain, S. (2023). Emerging Applications of Brain Computer Interfaces: A Comprehensive Review and Future Perspectives. In 2023 IEEE 11th Region 10 Humanitarian Technology Conference, 312-317.
Cite this article
Xiong,M. (2024). Brain-computer interface applications in the aging population with Alzheimer’s and Parkinson’s disease. Applied and Computational Engineering,81,47-55.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Machine Learning and Automation
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Young, M. J., Lin, D. J., & Hochberg, L. R. (2021). Brain–Computer interfaces in neurorecovery and neurorehabilitation. In Seminars in neurology, 41(02), 206-216.
[2]. Wolpaw, J. R., Millan, J. D. R., & Ramsey, N. F. (2020). Brain-computer interfaces: Definitions and principles. Handbook of clinical neurology, 168, 15-23.
[3]. Mudgal, S. K., Sharma, S. K., Chaturvedi, J., & Sharma, A. (2020). Brain computer interface advancement in neurosciences: Applications and issues. Interdisciplinary Neurosurgery, 20, 100694.
[4]. Jackson, A., & Zimmermann, J. B. (2012). Neural interfaces for the brain and spinal cord—restoring motor function. Nature Reviews Neurology, 8(12), 690-699.
[5]. Alzheimer’s Disease Fact Sheet, National Institute on Aging. URL: https://www.nia.nih.gov/health/alzheimers-and-dementia/alzheimers-disease-fact-sheet. Last Accessed: 2024/08/04.
[6]. GBD Compare, Institute for Health Metrics and Evaluation. URL: http://vizhub.healthdata.org/gbd-compare. Last Accessed: 2024/08/04.
[7]. Taya, F., Sun, Y., Babiloni, F., Thakor, N., & Bezerianos, A. (2015). Brain enhancement through cognitive training: a new insight from brain connectome. Frontiers in systems neuroscience, 9, 44-63.
[8]. Oh, S. J., & Ryu, J. N. (2018). The effect of brain-computer interface-based cognitive training in patients with dementia. Journal of the Korean Society of Physical Medicine, 13(4), 59-65.
[9]. Carelli, L., Solca, F., Faini, A., Meriggi, P., et, al. (2017). Brain‐computer interface for clinical purposes: Cognitive assessment and rehabilitation. BioMed research international, 2017(1), 1695290.
[10]. Lin, P. J., Ku, H. C., & Lin, L. L. (2024). Design and Development of Cognitive Training Systems Based on Extended Reality and BCI Technology. In 2024 IEEE 7th Eurasian Conference on Educational Innovation, 4-7.
[11]. Denggui, F., Suyu, L., Zhihui, W., Qingyun. W., (2015). The control effect of deep brain stimulation on the dynamics of neuronal networks in Parkinson's disease (Chinese). In Proceedings of the 15th National Conference on Nonlinear Vibration and the 12th National Conference on Nonlinear Dynamics and Stability of Motion, 1.
[12]. Grimaldi, G., & Manto, M. (2010). Old and emerging therapies of human tremor. Clinical Medicine Insights: Therapeutics, 2, 2999.
[13]. Ferrazoli, N., Donadon, C., Rezende, A., Skarzynski, P. H., & Sanfins, M. D. (2022). The application of P300-long-latency auditory-evoked potential in Parkinson disease. International archives of otorhinolaryngology, 26(01), 158-166.
[14]. Rosenfeld, J. V., & Wong, Y. T. (2017). Neurobionics and the brain–computer interface: current applications and future horizons. Medical Journal of Australia, 206(8), 363-368.
[15]. Shi, T., Ren, L., & Cui, W. (2019). Feature extraction of brain–computer interface electroencephalogram based on motor imagery. IEEE Sensors Journal, 20(20), 11787-11794.
[16]. Ren, S., Wang, W., Hou, Z. G., Liang, X., Wang, J., & Shi, W. (2020). Enhanced motor imagery based brain-computer interface via FES and VR for lower limbs. IEEE Transactions on Neural Systems and Rehabilitation Engineering, 28(8), 1846-1855.
[17]. Chen, X., Wang, Y., Nakanishi, M., Gao, X., Jung, T. P., & Gao, S. (2015). High-speed spelling with a noninvasive brain–computer interface. Proceedings of the national academy of sciences, 112(44), E6058-E6067.
[18]. Ebrahimi, T., Vesin, J. M., & Garcia, G. (2003). Brain-computer interface in multimedia communication. IEEE signal processing magazine, 20(1), 14-24.
[19]. Lazarou, I., Nikolopoulos, S., Petrantonakis, P. C., Kompatsiaris, I., & Tsolaki, M. (2018). EEG-based brain–computer interfaces for communication and rehabilitation of people with motor impairment: a novel approach of the 21st Century. Frontiers in human neuroscience, 12, 14.
[20]. Benabid, A. L. (2003). Deep brain stimulation for Parkinson’s disease. Current opinion in neurobiology, 13(6), 696-706.
[21]. Yue, C. (2023). Privacy and Ethical Concerns of Brain-Computer Interfaces. In 2023 IEEE International Conference on Metaverse Computing, Networking and Applications, 134-138.
[22]. Limchesing, T., Chua, A., Shi, C., Baldovino, R., et, al. (2021). A review on recent applications of EEG-based BCI in wheelchairs and other assistive devices. In 2021 IEEE 13th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment, and Management, 1-6.
[23]. Karikari, E., & Koshechkin, K. A. (2023). Review on brain-computer interface technologies in healthcare. Biophysical Reviews, 15(5), 1351-1358.
[24]. Patel, N., Verma, J., & Jain, S. (2023). Emerging Applications of Brain Computer Interfaces: A Comprehensive Review and Future Perspectives. In 2023 IEEE 11th Region 10 Humanitarian Technology Conference, 312-317.