






1. Introduction
1.1. Background and motivation
Stroke, also known as cerebrovascular accident, is a significant health challenge that has far-reaching effects on affected individuals. The impact of stroke on the quality of life and function of patients is enormous. According to the World Health Organization, stroke is a leading cause of adult disability and mortality [1,2]. It can result in speech and motor impairments, and even paralysis, imposing a significant burden on patients and their families. Consequently, there is an urgent need to explore innovative treatment methods to aid in the recovery of stroke patients.
1.2. Importance of stroke treatment combine with Brain-Computer Interface(BCI)and Deep Learning(DL)
Integrating Deep Learning and BCI for Enhanced Treatment To further enhance the impact of BCI in stroke treatment, the integration of deep learning, a form of artificial intelligence, is imperative. Deep learning mimics the workings of the human brain, identifying patterns and making decisions through learning and training. By combining deep learning with BCI, it becomes possible to interpret brain signals more accurately and achieve finer control [3]. This paves the way for more personalized and precise rehabilitation strategies for stroke patients, enabling them to better reconstruct damaged neural connections and regain functional independence. In summary, the integration of deep learning and BCI technology presents an opportunity to provide more effective treatment for stroke patients. This paper aims to explore the application of deep learning-based BCI in stroke treatment, with the goal of offering new breakthroughs and hope for the rehabilitation of stroke patients.
1.3. Objectives and structure of the paper
The aim of this review is to summarize the ways in which the combination of deep learning and brain-computer interface (BCI) technologies can aid in the rehabilitation of stroke patients. This paper gathers studies that have assessed the intersection of deep learning and BCI for stroke subjects, evaluates the methodological quality of these studies, and examines the relationship between the interventions' effects and the rehabilitation outcomes achieved. Additionally, the review addresses the shortcomings in current research and outlines potential future directions for the integration of deep learning in stroke rehabilitation using BCI technologies.
2. Application of DL-Based BCI Used in the Field of Brain Stroke Detection and Diagnosis
2.1. Stroke detection using MRI signals
MRI is one of the most used techniques in stroke diagnosis. Therefore, some researchers used MRI signals to detect the stroke using some deep learning techniques.
Vascular regional classification is an important part of stroke diagnosis. A research team applied deep learning technology to accurately classify different types of strokes such as middle cerebral artery stroke, posterior circulation stroke, and watershed stroke, by automatically extracting vascular features [4]. Researchers applied a transfer learning method based on MobileNetV2 and EfficientNet-B0 CNN architecture. In terms of stroke detection, the modified MobileNetV2 and EfficientNet-B0 models achieved 96% (κ: 0.92) and 93% (κ: 0.86) accuracy, respectively. In terms of vascular region, the modified MobileNetV2 and EfficientNet-B0 models achieved 93% (κ: 0.895) and 87% (κ: 0.805) accuracy, respectively.
To detect and respond to strokes in their early stages. Researchers applied different deep learning method in strokes detection field. researchers paid more attention to early recognition of ischemic stroke [5]. They used several pre-trained CNN models to process the datasets. Then they combined support vector machine (SVM) classifiers and iterative majority voting (IMV) methods to detect ischemic acute infarction. The proposed method achieved an accuracy of 97.93% on the collected dataset, with an F1-Score of 97.98%, a precision of 99.07%, and a recall rate of 96.93%.
Another research team analyzed the MRI image dataset and utilized traditional machine learning methods and deep learning methods in stroke diagnosis [6]. For the MRI image dataset, the researchers applied Alexnet and a hybrid model of Alexnet+SVM. The Alexnet model contained 25 layers, including 5 convolution layers, 3 Maximum pooling layers, and 3 full connect layers. The Alexnet+SVM model achieved 99.9% accuracy, 100% sensitivity, and 99.80% specificity on MRI image datasets. The hybrid model performed better on MRI datasets than the AlexNet model alone.
2.2. Stroke detection using EEG signal
Although MRI is very effective in stroke recognition, it is not very convenient for patients to use. Therefore, some researchers try to use EEG to detect strokes. A research team collected one-minute resting-state EEG data from stroke patients [7]. Researchers constructed various deep-learning models for different tasks which includes identifying stroke type, involved artery, and stroke severity. Among them, the stroke-type classification model achieved an accuracy of 97.74% and an F1 score of 0.9774. The stroke severity assessment model achieved a correlation coefficient of 0.91, showing a high correlation. The affected artery classification model used 33 features to achieve an accuracy of 95.7% with a 0.9482 F1 score. Another research team collected data from 7 healthy subjects and 7 stroke patients [8]. They designed an EEG-CNN deep learning network with four layers. It is found that theαrhythm EEG in the MI task has the highest discrimination, and the average accuracy of the EEG-CNN network model is 79.0%, which has obvious advantages in the prediction accuracy of EEG-CNN compared with other feature extraction and deep learning algorithms. The results of two studies demonstrate that the integration of EEG signals with deep learning algorithms can overcome the problem of low resolution in EEG signals. This consequence enables the practical application of EEG for stroke detection in real-life scenarios (see Fig.1).
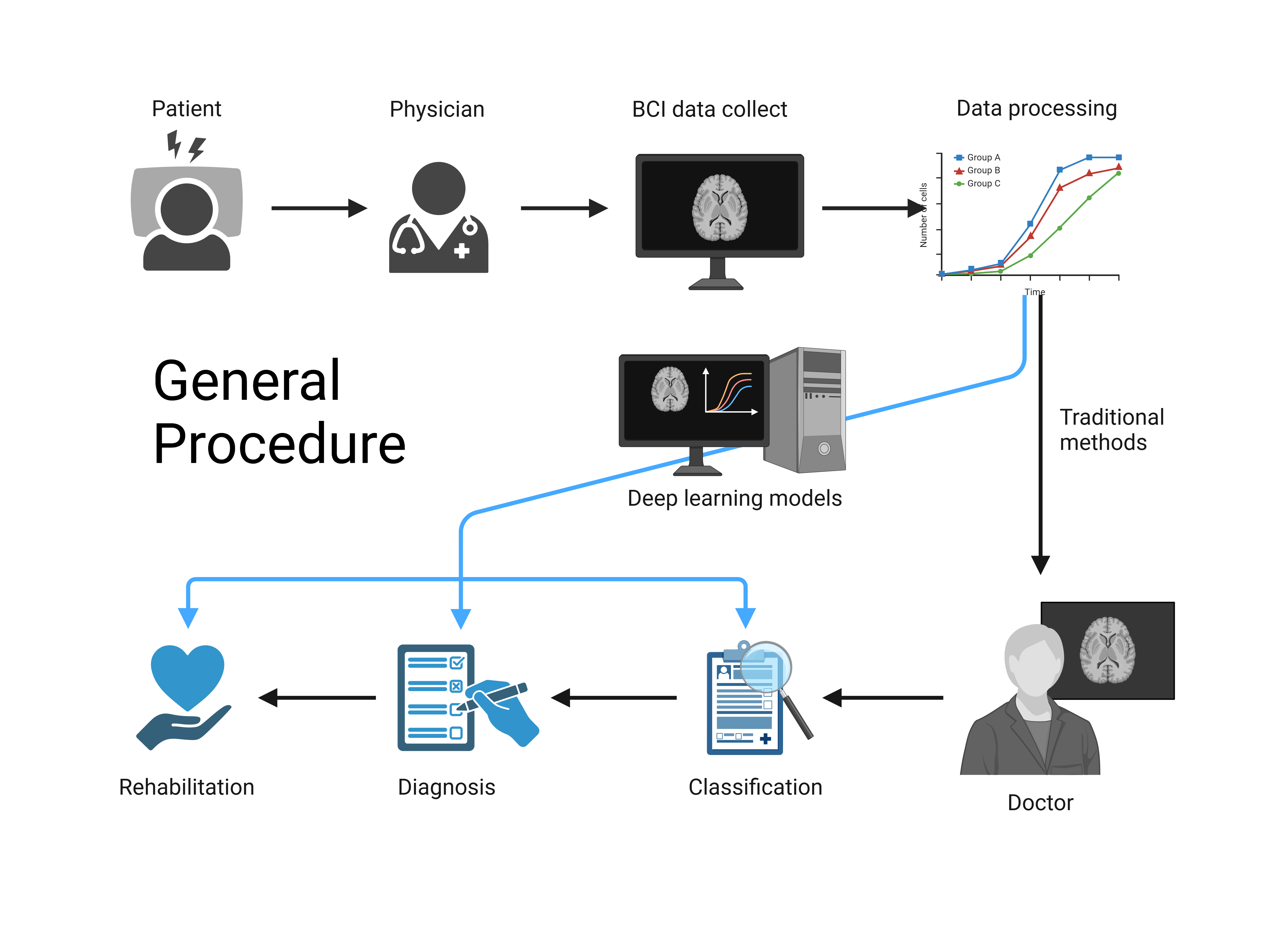
Figure 1. General procedure of deep learning based BCI.
3. Application of DL-Based BCI in Post-Stroke Rehabilitation
3.1. Motor rehabilitation
Motor rehabilitation after a stroke is a key component of the rehabilitation process for many patients, helping them regain as much motor function as possible, thereby improving their quality of life. Combining BCI and deep learning technology plays an important role in motor rehabilitation. The integration of BCI technology and traditional rehabilitation methods can enhance treatment efficacy by combining MI-BCI with standard arm therapy [9]. The Fugl Meyer Movement Assessment (FMA) score was used to monitor the progress of 13 stroke patients in the study at baseline (week 0), after intervention (week 6), and follow-up (weeks 12 and 24). Deep learning models analyses the electroencephalogram (EEG) data of patients during the treatment process, adjust and optimize the response of BCI in real-time, and maximize the therapeutic effect [10]. The stroke-specific FC patterns of patients with unilateral hemisphere stroke were studied. Calculate the partial correlation coefficients between multiple electroencephalogram (EEG) channels to construct a functional network of healthy control group and stroke patients. Then, deep learning-based graph analysis is used to characterize specific FC patterns in stroke patients. It is also common to improve data analysis accuracy by combining BCI with different deep-learning models [11]. The channel optimization process in EEG signal analysis for post-stroke treatment. Extract EEG signals into different frequency bands through wavelet transform. Then, a genetic algorithm is used to optimize the channel, reduce redundancy, and improve data processing efficiency. Using a Convolutional Neural Network (CNN) to classify optimized channels significantly improved the classification accuracy from 66.67% to 93.33%. Similarly, Principal Component Analysis (PCA) extracts signals by reducing the information of each channel, rather than focusing on the extracted features [12]. The EEG signals of post-stroke patients were also analysed using wavelet transform, PCA, and recurrent neural network (RNN). The wavelet transforms extract key frequency components including Delta, Theta, Alpha, and Mu waves to distinguish stroke conditions. Then PCA is used to reduce the dimensionality of multi-channel EEG data, preserve basic information, and minimize redundancy. The classification accuracy was significantly improved from 60% to 86% through PCA. Another group of researchers also applied a similar approach in their research[13], combining Common Space Pattern (CSP) filtering with Linear Discriminant Analysis (LDA) classifiers for different channel configurations to ensure high accuracy in the smallest possible channel. Through this adjustment, although CSP did not significantly improve classification performance with fewer channels, its application to 45 electrodes still greatly improved accuracy, achieving an AU-ROC curve of 0.90.
In addition, K K. In Ang and C. Guan's article [14], they used fixed models to help patients learn and control specific EEG features to complete tasks such as cursor control and arm orthotics. Machine learning methods construct models for topics based on calibrated session data to facilitate rapid BCI deployment and effectively detect motion images (MI) with high precision. The adaptive strategy continuously updates these models’ using data from calibration and feedback sessions to address the nonstationary between sessions, demonstrating a significant improvement in MI detection accuracy. Clinical trials have demonstrated the feasibility and effectiveness of these strategies, particularly machine learning methods, in improving motor function in stroke patients, as evidenced by the significant improvement in Fugl Meyer motor assessment scores.
3.2. Neural rehabilitation
The application of neural rehabilitation also reflects the diversity and innovation of technology integration [15]. Due to the non-stationary nature of EEG signals, brain-computer interfaces often require frequent calibration, leading to inconsistency between sessions and hindering their widespread application in rehabilitation. To address this issue, researchers have explored domain adaptation and deep learning techniques, particularly using the EEGNet architecture to design uncalibrated BCIs. EEGNet's ability to perform interdisciplinary classification of motion image tasks using data from hemiplegic stroke patients has shown promise, achieving performance comparable to traditional feature engineering methods. This method reduces the reliance on feature engineering and subject-specific tuning, allowing brain-computer interfaces to learn directly from raw EEG data. The study emphasizes that these advancements can improve the usability of brain-computer interfaces in neurorehabilitation, providing patients with consistent and immediate feedback, thereby reducing frustration and enhancing motivation during the rehabilitation process.
In addition, advanced neurorehabilitation methods, particularly gait rehabilitation that combines robot-assisted training with physical therapy [16]. By providing structured and repetitive training modes to enhance gait recovery in stroke patients, as well as epidural electrical stimulation (EES) to awaken walking patterns through electrical stimulation of the spinal cord, it is expected to restore movement after spinal cord injury. This study emphasizes the usage of brain-computer interfaces (BCI) to decode motor or cognitive intentions from brain activity, converting these predictions into commands for robotic devices, thereby enabling users to participate more actively in rehabilitation. At the same time, the use of Long Short-Term Memory (LSTM) networks was validated, which can accurately decode gait phases from EEG signals, indicating their real-time application potential in neural prosthesis devices and providing more natural motion control for patients with nerve injuries.
An innovative stroke rehabilitation method combines motion imaging (MI) with brain-computer interface (BCI) technology and virtual reality (VR) feedback to enhance neural reorganization and motor recovery [17]. Patients imagine moving their body parts and capturing their neural activity through electroencephalography. The system uses deep learning algorithms to classify these signals in real time. VR games provide immersive feedback, where successful imagined actions generate virtual actions, such as exploding targets. This method aims to make rehabilitation more attractive and effective and improve patient motivation and overall treatment outcomes.
4. Conclusion
4.1. Application of DL-Based BCI technology in stroke detection
The introduction of deep learning has significantly improved the capability of BCI in stroke detection. Specifically, deep learning models such as convolutional neural networks (CNNS) show superior classification and recognition capabilities when processing complex MRI and EEG signals. These models not only improve the classification accuracy of stroke types and damaged brain areas, but also perform well in early stroke recognition, thus guaranteeing timely treatment. The application of deep learning effectively overcomes the problem of low signal resolution in traditional methods, making the clinical application of BCI technology in the field of stroke detection a reality.
4.2. Application of BDL-CI technology bn stroke rehabilitation
In terms of rehabilitation treatment, the combination of deep learning and BCI provides patients with more accurate and personalized rehabilitation programs. By analyzing the patient's electroencephalogram (EEG) data in real time, the deep learning model can optimize the feedback mechanism of the BCI system to maximize the effectiveness of rehabilitation training. The application of this technology not only significantly improves the patient's motor function recovery, but also improves the efficiency of data processing by reducing multi-channel data redundancy. In addition, uncalibrated BCI systems supported by deep learning also show significant advantages in reducing frustration during patient recovery and enhancing treatment continuity.
4.3. Future and risk consideration
Although deep learning and BCI technologies show great potential in stroke detection and rehabilitation, their widespread application still faces many challenges and risks. First, the dependence of deep learning models on large-scale, high-quality data may limit their application in data-poor environments. Second, the complexity and high cost of the BCI system may be a barrier to its adoption in resource-limited healthcare Settings. Future research should aim to develop more efficient and low-cost methods of data acquisition and processing to enhance the accessibility and universality of the technology. In addition, with the mass collection and processing of patient data, data privacy and security issues have become important issues to be solved. Future research should pay more attention to the development of data encryption and anonymization technology to ensure the security and privacy of patient information, and further promote the safe application of BCI technology in stroke rehabilitation. After the discussion in this paper, the combination of deep learning and BCI technology has significantly improved the technical level of stroke detection and rehabilitation. This technology integration not only improves the accuracy of detection, but also enhances the personalization and effectiveness of the rehabilitation process. Despite the current challenges and risks, with the continuous progress of technology, the application of deep learning and BCI technology in stroke treatment is still promising. Future research should continue to optimize these technologies and promote their widespread application in clinical practice to provide more comprehensive and efficient rehabilitation programs for stroke patients.
Acknowledgments
Xiyang Lin, Canyu Yang, Weihang Yuan, and Caizhou Tao contributed equally to this work and should be considered co-first authors.
References
[1]. R.G. Nogueira, A.P. Jadhav, D.C. Haussen, et al., Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct, N. Engl. J. Med. 378 (1) (2018) 11–21, https://doi.o rg/10.1056/NEJMoa1706442.
[2]. G.W. Albers, M.P. Marks, S. Kemp, et al., Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging, N. Engl. J. Med. 378 (8) (2018) 708–718, https://doi.org/10.1056/NEJMoa1713973.
[3]. S. Al-Shoukry, T. H. Rassem and N. M. Makbol, “Alzheimer’s diseases detection by using deep learning algorithms: A mini-review,” IEEE Access, vol. 8, pp. 77131–77141, 2020.
[4]. Y. K. Cetinoglu, I. O. Koska, M. E. Uluc, and M. F. Gelal, "Detection and vascular territorial classification of stroke on diffusion-weighted MRI by deep learning," European Journal of Radiology, vol. 145, 2021, Art. no. 110050.
[5]. B. Tasci, "Automated ischemic acute infarction detection using pre-trained CNN models' deep features," Biomedical Signal Processing and Control, vol. 82, 2023, Art. no. 104603.
[6]. Z. G. Al-Mekhlafi, E. M. Senan, T. H. Rassem, B. A. Mohammed, N. M. Makbol, A. A. Alanazi, et al., "Deep learning and machine learning for early detection of stroke and haemorrhage," Computers, Materials and Continua, vol. 72, no. 1, pp. 775-796, 2022.
[7]. S. Singh, D. Dawar, E. Mehmood, J. D. Pandian, R. Sahonta, S. Singla, et al., "Determining Diagnostic Utility of EEG for Assessing Stroke Severity using Deep Learning Models," Biomedical Engineering Advances, vol. 7, 2024, Art. no. 100121.
[8]. J. Ma, et al., "Stroke Identification Based on EEG Convolutional Neural Network," in Intelligent Life System Modelling, Image Processing and Analysis (LSMSIS ICSEE 2021), M. Fei, L. Chen, S. Ma, and X. Li, eds., vol. 1467, Singapore: Springer, 2021, pp. 266-275.
[9]. R. Foong et al., "Assessment of the Efficacy of EEG-Based MI-BCI With Visual Feedback and EEG Correlates of Mental Fatigue for Upper-Limb Stroke Rehabilitation," IEEE Transactions on Biomedical Engineering, vol. 67, no. 3, pp. 786-794, March 2020.
[10]. C. Zhao, R. Li, C. Wang, W. Huang, and Y. Zhang, "EEG-Based Brain Network Analysis in Stroke Patients During a Motor Execution Task," in Proc. 9th Int. IEEE EMBSConf. Neural Eng., San Francisco, CA, USA, March 20-23, 2019, pp. 887-890
[11]. H. R. Yasin, E. C. Djamal, and F. Nugraha, "Optimization of Multi-Channel EEG Signal Using Genetic Algorithm in Post-Stroke Classification," in 2020 3rd International Conference on Computer and Informatics Engineering (IC2IE), Bali, Indonesia, 2020, pp. 129-134,
[12]. A. S. Ananda, E. C. Djamal, and F. Nugraha, "Post-Stroke Recognition Based on EEG Using PCA and Recurrent Neural Networks," 2020 3rd International Conference on Computer and Informatics Engineering (IC2IE), 2020, pp. 1-7,
[13]. C. Tangwiriyasakul, V. Mocioiu, M. J. A. M. van Putten, and W. L. C. Rutten, "Classification of motor imagery performance in acute stroke," J. Neural Eng., vol. 11, no. 3, pp. 1-9, 2014,
[14]. K. K. Ang and C. Guan, "EEG-Based Strategies to Detect Motor Imagery for Control and Rehabilitation," IEEE Transactions on Neural Systems and Rehabilitation Engineering, vol. 25, no. 4, pp. 392-401, April 2017,
[15]. H. Raza, A. Chowdhury, and S. Bhattacharyya, "Deep Learning based Prediction of EEG Motor Imagery of Stroke Patients for Neuro-Rehabilitation Application," in Proceedings of the International Joint Conference on Neural Networks (IJCNN), 2020, pp. 1-8.
[16]. S. Tortora, S. Ghidoni, C. Chisari, S. Micera, and F. Artoni, "Deep learning-based BCI for gait decoding from EEG with LSTM recurrent neural network," Journal of Neural Engineering, vol. 17, no. 4, pp. 046011, Jul. 2020,
[17]. T. Karácsony, J. P. Hansen, H. K. Iversen, and S. Puthusserypady, "Brain Computer Interface for Neuro-rehabilitation With Deep Learning Classification and Virtual Reality Feedback," in Proceedings of the Augmented Human International Conference 2019 (AH2019), Reims, France, 2019, pp. 1-8,
Cite this article
Lin,X.;Yang,C.;Yuan,W.;Cai,Z. (2025). The Application of BCI Based on Deep Learning in Stroke Treatment. Applied and Computational Engineering,131,1-7.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Machine Learning and Automation
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. R.G. Nogueira, A.P. Jadhav, D.C. Haussen, et al., Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct, N. Engl. J. Med. 378 (1) (2018) 11–21, https://doi.o rg/10.1056/NEJMoa1706442.
[2]. G.W. Albers, M.P. Marks, S. Kemp, et al., Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging, N. Engl. J. Med. 378 (8) (2018) 708–718, https://doi.org/10.1056/NEJMoa1713973.
[3]. S. Al-Shoukry, T. H. Rassem and N. M. Makbol, “Alzheimer’s diseases detection by using deep learning algorithms: A mini-review,” IEEE Access, vol. 8, pp. 77131–77141, 2020.
[4]. Y. K. Cetinoglu, I. O. Koska, M. E. Uluc, and M. F. Gelal, "Detection and vascular territorial classification of stroke on diffusion-weighted MRI by deep learning," European Journal of Radiology, vol. 145, 2021, Art. no. 110050.
[5]. B. Tasci, "Automated ischemic acute infarction detection using pre-trained CNN models' deep features," Biomedical Signal Processing and Control, vol. 82, 2023, Art. no. 104603.
[6]. Z. G. Al-Mekhlafi, E. M. Senan, T. H. Rassem, B. A. Mohammed, N. M. Makbol, A. A. Alanazi, et al., "Deep learning and machine learning for early detection of stroke and haemorrhage," Computers, Materials and Continua, vol. 72, no. 1, pp. 775-796, 2022.
[7]. S. Singh, D. Dawar, E. Mehmood, J. D. Pandian, R. Sahonta, S. Singla, et al., "Determining Diagnostic Utility of EEG for Assessing Stroke Severity using Deep Learning Models," Biomedical Engineering Advances, vol. 7, 2024, Art. no. 100121.
[8]. J. Ma, et al., "Stroke Identification Based on EEG Convolutional Neural Network," in Intelligent Life System Modelling, Image Processing and Analysis (LSMSIS ICSEE 2021), M. Fei, L. Chen, S. Ma, and X. Li, eds., vol. 1467, Singapore: Springer, 2021, pp. 266-275.
[9]. R. Foong et al., "Assessment of the Efficacy of EEG-Based MI-BCI With Visual Feedback and EEG Correlates of Mental Fatigue for Upper-Limb Stroke Rehabilitation," IEEE Transactions on Biomedical Engineering, vol. 67, no. 3, pp. 786-794, March 2020.
[10]. C. Zhao, R. Li, C. Wang, W. Huang, and Y. Zhang, "EEG-Based Brain Network Analysis in Stroke Patients During a Motor Execution Task," in Proc. 9th Int. IEEE EMBSConf. Neural Eng., San Francisco, CA, USA, March 20-23, 2019, pp. 887-890
[11]. H. R. Yasin, E. C. Djamal, and F. Nugraha, "Optimization of Multi-Channel EEG Signal Using Genetic Algorithm in Post-Stroke Classification," in 2020 3rd International Conference on Computer and Informatics Engineering (IC2IE), Bali, Indonesia, 2020, pp. 129-134,
[12]. A. S. Ananda, E. C. Djamal, and F. Nugraha, "Post-Stroke Recognition Based on EEG Using PCA and Recurrent Neural Networks," 2020 3rd International Conference on Computer and Informatics Engineering (IC2IE), 2020, pp. 1-7,
[13]. C. Tangwiriyasakul, V. Mocioiu, M. J. A. M. van Putten, and W. L. C. Rutten, "Classification of motor imagery performance in acute stroke," J. Neural Eng., vol. 11, no. 3, pp. 1-9, 2014,
[14]. K. K. Ang and C. Guan, "EEG-Based Strategies to Detect Motor Imagery for Control and Rehabilitation," IEEE Transactions on Neural Systems and Rehabilitation Engineering, vol. 25, no. 4, pp. 392-401, April 2017,
[15]. H. Raza, A. Chowdhury, and S. Bhattacharyya, "Deep Learning based Prediction of EEG Motor Imagery of Stroke Patients for Neuro-Rehabilitation Application," in Proceedings of the International Joint Conference on Neural Networks (IJCNN), 2020, pp. 1-8.
[16]. S. Tortora, S. Ghidoni, C. Chisari, S. Micera, and F. Artoni, "Deep learning-based BCI for gait decoding from EEG with LSTM recurrent neural network," Journal of Neural Engineering, vol. 17, no. 4, pp. 046011, Jul. 2020,
[17]. T. Karácsony, J. P. Hansen, H. K. Iversen, and S. Puthusserypady, "Brain Computer Interface for Neuro-rehabilitation With Deep Learning Classification and Virtual Reality Feedback," in Proceedings of the Augmented Human International Conference 2019 (AH2019), Reims, France, 2019, pp. 1-8,