






1. Introduction
Communication between humans and computers has been a popular research topic in recent years. Modern brain-computer interface (BCI) technology enables humans to interact with computers or other external devices by directly decoding neural signals from the brain. BCI was first proposed in the 1970s. Researchers in this field have been motivated by two main factors: establishing a new output pathway for severely disabled patients and expanding human direct control over external systems. Driven by these goals, they have actively engaged in this innovative and challenging research. Scientists initially conducted experiments on animals to establish a direct communication pathway between the brain and the external environment. Subsequently, two pioneering studies demonstrated how the BCI system could control a neuroprosthetic arm and achieve arm movement recovery after paralysis. Ajiboye et al. confirmed the effectiveness of intracortical BCI systems in rehabilitation for patients with limb impairments [1].
Brain-computer interface (BCI) technology has permeated many areas of our daily lives. In the field of medical rehabilitation, BCI is used for neural rehabilitation, prosthetic control, and motor function recovery, helping patients with stroke, spinal cord injuries, and amyotrophic lateral sclerosis (ALS) regain movement and communication abilities. In the domain of assistive communication, BCI provides communication tools for individuals with severe motor impairments (such as locked-in syndrome), enabling them to control text input or speech synthesis devices through brain signals. In neuroscience research, BCI is employed to study brain function, neural signal processing, and cognitive behavior, aiding in a deeper understanding of neural mechanisms. In the application of smart prosthetics and exoskeletons, BCI enables precise control of prosthetic limbs or exoskeletons through brain signals, significantly enhancing the mobility of patients. In human-computer interaction, BCI is widely applied in virtual reality (VR), augmented reality (AR), and gaming, providing users with a more immersive and natural interactive experience.
2. Literature review
2.1. Basic principles of brain-machine interface
The definition of brain-machine interface technology provided at the first International BCI Conference is: "A brain-computer interface is a communication system that does not depend on the normal output path composed of peripheral nerves and muscles." [2] Brain-machine interface technology collects brain wave signals from various brain function areas based on their location and depth, performs a series of data processing tasks, and ultimately achieves decoding of brain activity states or intentions. During signal collection, the subject either passively receives stimulation or actively engages in thinking and neural activities, producing brain wave signals containing information about the characteristics of those activities. Subsequently, through brain wave signal processing (feature extraction), the continuous analog signals are converted into digital signals represented by feature parameters, allowing the computer to read and analyze them and determine the corresponding brain thought activities to generate operational commands. The final output signal controls the manipulative device as a control command [3].
2.2. Classification of brain-computer interface systems by signal acquisition method
Brain-computer interfaces (BCIs) can be categorized into three types based on different signal acquisition methods: non-invasive, partially invasive, and invasive BCIs.
2.2.1. Non-invasive BCI
The first type is Non-invasive BCI, which acquires brain signals by placing electrodes on the scalp (such as electroencephalography, EEG) or using other external devices (such as magnetoencephalography, MEG, and functional near-infrared spectroscopy, fNIRS). This method is safe, non-intrusive, and does not require surgery, making it suitable for most situations. However, since the signals must pass through the scalp, skull, and other tissue layers, the signal strength is weaker and more susceptible to noise interference. This approach is mainly applied in technologies like EEG, fNIRS, and MEG [4]. In the field of non-invasive brain-computer interfaces (BCIs), BrainCo has developed the BrainRobotics intelligent bionic hand, which was approved for market release by the U.S. Food and Drug Administration (FDA) in 2022. This high-tech assistive device integrates BCI technology with artificial intelligence algorithms. It is capable of recognizing the wearer’s electromyographic and neuroelectrical signals from the arm, enabling upper limb amputees to control the intelligent bionic hand as if it were their natural limb [5].
In terms of invasive BCIs, researchers have enabled a patient with upper body paralysis to manipulate a robotic arm using a BCI to independently eat with a knife and fork. A minimally invasive BCI using three intracranial electrodes has achieved a typing speed of 12 words per minute. Neuralink's product is expected to enter clinical trials within the next six months, while products from companies such as Synchron and Shanghai BrainTiger Neurotech Co., Ltd. are currently undergoing clinical trials [6].
2.2.2. Partially Invasive BCI
The second type is Partially Invasive BCI, which acquires higher-quality signals by placing electrodes between the skull and the cerebral cortex (such as electrocorticography, ECoG). This method carries lower surgical risk and strikes a balance between signal quality and safety. It is typically used in scenarios that demand higher signal quality but where fully invasive methods are not suitable [7].
2.2.3. Invasive BCI
The third type is Invasive BCI, which requires surgical implantation of electrodes directly into the cerebral cortex or neural tissue. This method can capture high-resolution, high signal-to-noise ratio neural signals, enabling more precise control and broader applications, especially in scenarios requiring highly accurate neural control (such as prosthetic limb control). However, invasive methods carry surgical risks, the potential for infection, and biocompatibility concerns with electrode materials [8].
Among the three signal acquisition methods, non-invasive brain-computer interface (BCI) technology is currently the most widely used. However, due to the placement of devices on the surface of the brain, the signal clarity is relatively low, though the method is non-invasive. Nowadays, there are various non-invasive devices available, each with its own advantages and disadvantages depending on different considerations. Among them, EEG devices are the most recommended as they facilitate remote diagnosis by expert physicians. There are various types of EEG devices on the market, differing in the number of electrodes, cost, and intended applications.The primary application of electroencephalography (EEG) is the study of brain disorders such as epilepsy. If no signals are detected through EEG monitoring, the brain is considered to be in a state of brain death. For example, a brain functional map, as shown in the above figure, can be obtained using EEG.
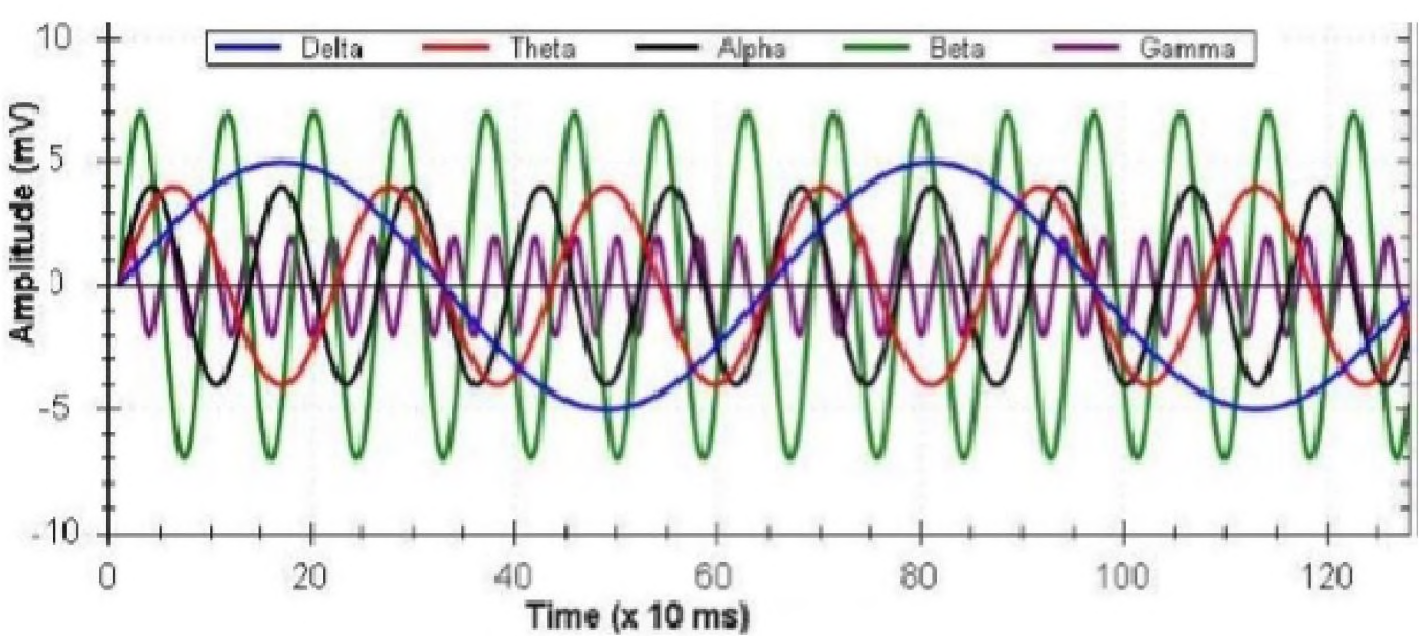
Figure 1: The five frequency bands and their relationship (see online version for colours)
2.3. Application of brain-computer interface
2.3.1. Clinical rehabilitation application in medicine
The clinical rehabilitation application of brain-computer interface in medicine mainly includes two aspects: Firstly, the brain-computer interface can convert the acquired feature signal instructions into continuous and multi-dimensional precise control of exoskeleton or functional electrical stimulation (FES). The assistive BCI can help patients better use these devices in their daily life and work, thereby improving their quality of life. Secondly, the brain-computer interface can activate the neural plasticity of the brain by decoding the EEG signals of the patient and providing real-time feedback during training, thereby helping the patient improve their motor relearning ability. This type of brain-computer interface is called rehabilitation BCI. Currently, the brain-computer interface technology used for hand function rehabilitation after stroke in clinical practice is mostly based on motor imagery, which belongs to non-invasive brain-computer interface. By wearing an electrode cap and applying conductive cream on the scalp, the brain signals are collected and feature processing is performed to control the external devices of the brain-computer interface, without causing complications. For patients with a history of epilepsy, since the brain-computer interface mainly relies on EEG signals for analysis, and EEG is an effective method for monitoring epilepsy, there is no contradiction between the brain-computer interface rehabilitation and epilepsy. The brain-computer interface-based rehabilitation training itself does not directly affect the physiological changes of the patient, and blood pressure instability, heart rate instability, etc. caused by long-term sitting and persistent training are not attributed to contraindications of the brain-computer interface. Of course, patients with severe complications and serious diseases such as heart, liver, and kidney are not suitable for this training. During brain-computer interface rehabilitation training, the patient needs to maintain a long-term interactive task with the computer screen and actively participate in the training, which may not form a good training atmosphere for patients with poor self-control and poor physical condition, such as those who cannot sit for a long time.
2.3.2. Applications in other fields
In the field of leisure and entertainment, software and games developed by combining brain-computer interface and virtual reality technology can provide a brand new entertainment experience. Players can immerse themselves in the game environment and enjoy the feeling of being there, expanding the boundaries of entertainment and achieving unprecedented experiences; In the field of factory operation, brain-computer interface technology can be used to control mechanical equipment, especially in deep sea, space or other dangerous environments, thus avoiding personnel from performing dangerous operations personally; In the military field, brain-computer interface technology can be used to achieve unmanned operation and brain-controlled machine execution of military strikes, accurately attacking designated targets and completing military tasks, and also by brain-controlling animals to spy on the military bases and facilities of the enemy's battlefield.
3. Challenges and responses in brain-computer interface technology
BCI technology has a history of over 50 years of development from the 1970s to the present, but because its research started later, it is more technically complex and involves multiple disciplines, so there are still many difficulties and challenges in its practical application. The main challenges currently faced by BCI technology include the accuracy and stability of signal acquisition, the complexity of data processing and decoding algorithms, user adaptability and learning curve, ethical issues, etc. This paper will focus on detailed research on signal acquisition, decoding algorithms, and ethical and moral issues.
3.1. Signal acquisition
At present, the feature extraction and classification technologies used in BCI technology are not able to fully correctly reflect the requirements of the patient's thought activities. During the signal acquisition process, various external factors will affect the accuracy of the acquired signal: the individual random factors of the subject, such as emotions, attention concentration degree, stimulus response degree differences, will comprehensively affect the accuracy of the BCI system; in addition, the subject's training level, signal analysis and processing methods, classification identification results, etc. will also affect the output accuracy.
The latest research results have demonstrated the development of high-resolution electrode arrays, which use nanomaterial-made flexible and miniaturized electrodes. Such electrodes can better adhere to the surface of the brain and reduce noise generation, thereby improving the resolution and stability of the source signal acquisition; optical imaging technology is also helpful for source signal acquisition today, such as optical coherence tomography (OCT), a new method for monitoring neural activity. OCT has high resolution and penetration depth, and has become a promising signal acquisition means for BCI; functional high-precision magnetic resonance imaging (fMRI) technology is another, which can be used in combination with EEG signals to provide more abundant brain activity data. This multi-modal fusion technology can better locate and understand the functional regions of the brain.
3.2. Data processing and decoding algorithms
The BCI (brain-computer interface) technology also faces many challenges in signal processing and decoding algorithms. Firstly, the EEG signal is inherently highly complex and non-linear. Secondly, the EEG signal has high temporal and spatial variability. In order to accurately decode these signals, the decoding algorithm must have high flexibility and adaptability. Furthermore, the decoding algorithm also faces real-time requirements. BCI systems usually need to process and decode EEG signals within milliseconds to provide real-time feedback. This places high demands on the algorithm's computational efficiency. While ensuring high-precision decoding, the algorithm's computational speed also needs to be optimized to meet the real-time processing requirements. Optimizing the algorithm's speed is a multi-level task, including model simplification and optimization, parallel computing, and hardware acceleration, etc. By using lightweight algorithms and hardware acceleration, modern BCI systems can operate in real-time scenarios, such as real-time gesture recognition, prosthetic control, with response times reduced to the millisecond level; the application of deep learning in BCI is also becoming increasingly widespread, especially in complex pattern recognition tasks, where deep learning algorithms have achieved significant progress in real-time EEG decoding applications, such as successful applications in epileptic seizure prediction, emotion recognition, and intent decoding.
Neuralink's founder, Elon Musk, demonstrated their invasive brain-computer interface system in August 2020, showing how their high-density electrode array communicates with a pig's brain, which can simultaneously obtain signals from a large number of neurons and transmit them to external devices at a very high rate through advanced wireless transmission technology, to control complex devices such as computers or prosthetics. While the research did not specify the rate, it is highly likely to exceed 1,000 bits per second, and the rate may be further increased in future application scenarios.
3.3. Ethical and moral issues
The progress of neural technology is amazing, as it has made many things that people could only dream of before a reality while also raising a number of ethical and moral issues for the world to consider. When a BCI system is installed, human thoughts and ideas are no longer limited to within the brain, but are extended to the external world through the BCI system, allowing thoughts to freely move and expand in an infinite space. This raises a series of issues, such as privacy issues: BCI systems collect and decode brain signals to obtain users' thoughts, emotions, and intentions. These data are highly sensitive and may contain personal privacy. If they are misused or leaked without permission, they can cause serious privacy violations; safety issues: On the one hand, implantable brain-computer interface technology can cause harm from implant surgery, and inserting electrodes into the brain can cause damage. On the other hand, long-term use of certain brain regions or neural pathways may cause uncertain harm; autonomy issues: Highly precise BCI technology may be abused to influence or control individuals' thoughts and behaviors, undermining their autonomy and making them slaves; responsibility issues: Who should bear the responsibility for the harm caused by machine malfunctions to oneself and society, etc.Therefore, we need to take some corresponding measures in the area of ethics. Develop and improve relevant laws and regulations: Develop special privacy protection laws for brain data, ensuring that users' EEG data are strictly protected. Establish informed consent regulations, requiring BCI systems to obtain users' informed consent before use. Establish a clear legal framework to clarify responsibility allocation and protect users' rights; Ethical considerations in technology design and development: Adopt data encryption and anonymous processing technologies in BCI design to minimize the risk of privacy leaks. Conduct comprehensive ethical evaluations before the launch of the technology and ensure that users have complete control over the technology to prevent its misuse; International cooperation and standard setting: Develop global BCI technology ethical standards and best practices, establish cross-border regulatory mechanisms, coordinate regulatory monitoring across countries, and prevent inconsistencies and spread of ethical issues due to regional differences.
3.4. Future trends of brain-computer interface
To promote market growth, investment needs to be increased. Venture capital and corporate investment in the BCI field will continue to rise, especially in startups and innovative technologies. These investments will further drive the research and commercialization of the technology. As the technology matures and applications expand, the brain-computer interface (BCI) market is expected to continue growing. According to market research reports, the demand for BCI in the medical, consumer electronics, and entertainment sectors is increasing.
Furthermore, BCI technology is expected to achieve further breakthroughs in healthcare. On one hand, in rehabilitation and prosthetic control, BCI technology is gradually maturing, with brain-controlled prosthetics and exoskeleton devices starting to commercialize, providing better functional recovery options for amputees and paralyzed patients. On the other hand, BCI technology is also being applied to treat neurological diseases such as epilepsy and Parkinson's disease, alleviating symptoms or improving patients' quality of life through deep brain stimulation and brainwave regulation.
At the same time, BCI technology will enhance the level of consumer electronics and entertainment. Consumer electronic products controlled by BCI, such as brain-controlled games and virtual reality devices, are entering the market, providing users with new interaction methods and entertainment experiences. Finally, the application of BCI technology has also driven the development of augmented reality (AR) and virtual reality (VR), allowing users to control virtual environments directly with their thoughts, enhancing immersion and interaction.
4. Conclusion
Brain-computer interface (BCI) technology has developed rapidly in the past few decades, gradually moving from laboratory research to clinical applications and gradually entering the consumer market, where it is becoming better known and more widely discussed. However, the current state of BCI technology is not fully mature, and future research should specifically focus on the following areas. Firstly, applying artificial intelligence and machine learning to BCI, particularly in real-time signal processing, user adaptation, and personalized customization, can greatly enhance the flexibility and functionality of the device. Secondly, combining visual, tactile, and other sensory inputs, as well as motor intentions, in a multimodal BCI has the potential to enhance the system's natural interaction capabilities, making BCI more widely applicable in daily life. Finally, improvement of non-invasive technology: Research on how to design and implement simple, efficient, and versatile wireless invasive BCI devices.
References
[1]. Ajiboye, A. B., Willett, F. R., Young, D. R., Memberg, W. D., Murphy, B. A., Miller, J. P., Walter, B. L., Sweet, J. A., Hoyen, H. A., Keith, M. W., Peckham, P. H., Simeral, J. D., Donoghue, J. P., Hochberg, L. R., & Kirsch, R. F. (2017). Restoration of reaching and grasping movements through brain-controlled muscle stimulation in a person with tetraplegia: a proof-of-concept demonstration. Lancet (London, England), 389(10081), 1821–1830. https://doi.org/10.1016/S0140-6736(17)30601-3
[2]. Wolpaw, J. R., Birbaumer, N., McFarland, D. J., Pfurtscheller, G., & Vaughan, T. M. (2002). Brain–computer interfaces for communication and control. Clinical Neurophysiology, 113(6), 767–791.
[3]. Schalk C, Moran D, et al. The emerging world of motor neuroprosthetics: a neurosurgical perspective. Neurosurgery. 2006;59:1-14, with permission.)
[4]. Abiri R, Borhani S, Sellers EW, et al. A comprehensive review of EEG-based brain–computer interface paradigms. J Neural Eng 2019;16:011001.
[5]. Handelman DA, Osborn LE, Thomas TM, et al. Shared control of bimanual robotic limbs with a brain-machine interface for self-feeding. Front Neurorobot, 2022, 16: 918001
[6]. Liu D, Xu X, Li D, et al. Intracranial brain-computer interface spelling using localized visual motion response. Neuroimage, 2022, 258: 119363
[7]. Mestais CS, Charvet G, Sauter-Starace F, et al. WIMAGINE: wireless 64-channel ECoG recording implant for long term clinical applications. IEEE Trans Neural Syst Rehabil Eng 2015;23:10–21.
[8]. Zhao Z-P, Nie C, Jiang C-T, et al. Modulating brain activity with invasive brain–computer interface: a narrative review. Brain Sci 2023;13:134.
Cite this article
Yang,J. (2025). Challenges and Trends in Brain-Computer Interface Technology. Applied and Computational Engineering,152,56-62.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 3rd International Conference on Software Engineering and Machine Learning
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Ajiboye, A. B., Willett, F. R., Young, D. R., Memberg, W. D., Murphy, B. A., Miller, J. P., Walter, B. L., Sweet, J. A., Hoyen, H. A., Keith, M. W., Peckham, P. H., Simeral, J. D., Donoghue, J. P., Hochberg, L. R., & Kirsch, R. F. (2017). Restoration of reaching and grasping movements through brain-controlled muscle stimulation in a person with tetraplegia: a proof-of-concept demonstration. Lancet (London, England), 389(10081), 1821–1830. https://doi.org/10.1016/S0140-6736(17)30601-3
[2]. Wolpaw, J. R., Birbaumer, N., McFarland, D. J., Pfurtscheller, G., & Vaughan, T. M. (2002). Brain–computer interfaces for communication and control. Clinical Neurophysiology, 113(6), 767–791.
[3]. Schalk C, Moran D, et al. The emerging world of motor neuroprosthetics: a neurosurgical perspective. Neurosurgery. 2006;59:1-14, with permission.)
[4]. Abiri R, Borhani S, Sellers EW, et al. A comprehensive review of EEG-based brain–computer interface paradigms. J Neural Eng 2019;16:011001.
[5]. Handelman DA, Osborn LE, Thomas TM, et al. Shared control of bimanual robotic limbs with a brain-machine interface for self-feeding. Front Neurorobot, 2022, 16: 918001
[6]. Liu D, Xu X, Li D, et al. Intracranial brain-computer interface spelling using localized visual motion response. Neuroimage, 2022, 258: 119363
[7]. Mestais CS, Charvet G, Sauter-Starace F, et al. WIMAGINE: wireless 64-channel ECoG recording implant for long term clinical applications. IEEE Trans Neural Syst Rehabil Eng 2015;23:10–21.
[8]. Zhao Z-P, Nie C, Jiang C-T, et al. Modulating brain activity with invasive brain–computer interface: a narrative review. Brain Sci 2023;13:134.