






1.Introduction
As an online form of harassment and aggression, cyberbullying has become a significant concern in the digital age. With the rapid development of communication technology, cyberspace has been identified as a hazardous environment where bullying may occur among adolescents [1]. The current prevalence estimates indicate that the percentage of adolescents experiencing at least one cyberbullying incident during an academic year ranges from 9% to 49% [2]. As documented in previous Youth Internet Safety Surveys (YISS), the dramatic increase in reported cyberbullying incidents over the past five years is a cause for concern [3]. Adolescents, who frequently use digital technologies to communicate with peers, are especially susceptible to the harmful effects of cyberbullying [4]. Given the aforementioned circumstances, the selection of auxiliary strategies by victims of cyberbullying has become increasingly deserving of attention in recent years.
The significance of this research is its potential to enhance the understanding of the factors influencing recovery from cyberbullying and inform the development of more effective assistive strategies. By examining the relationship between recovery duration and the choice of recovery strategies, this study helps clarify whether the current approaches to addressing cyberbullying adequately meet the needs of victims. Additionally, the research findings may suggest future directions for developing assistive strategies, which can potentially improve support for cyberbullying victims and promote more effective recovery processes.
2.Literature Review
Consistently, research has demonstrated the negative impact of cyberbullying on victims’ mental health and well-being. It is also found that individuals involved in cyberbullying, as victims, bullies or bully-victims, face increased risks of anxiety, depressive symptoms and diminished overall well-being [5]. Besides, some research suggests that recovery from cyberbullying might be more prolonged compared to recovery from traditional bullying, which is potentially due to the invasive and enduring nature of online harassment [6].
In response to the ongoing harm caused by cyberbullying, victims may adopt various supportive strategies, such as seeking assistance from family members or counselling agencies. In literature, the influence of cultural factors on individuals’ coping strategies when confronted with cyberbullying is emphasised. For example, Hu et al. found that Chinese victims of cyberbullying with higher levels of individualist cultural orientation were more inclined to apply acceptance, reframing, and striving strategies, as well as avoidance and detachment strategies; while in contrast, those with higher levels of collectivist orientation tended to rely on family support, religion and spirituality, and private emotional outlets [7].
Despite these insights, the relationships between the duration of recovery from cyberbullying and the choice of recovery strategies remain inadequately explored. To address this gap, the current study aims to investigate the association between recovery length and the selection of assistive strategies when coping with cyberbullying experiences. Through utilising a quantitative research methodology and collecting data through questionnaires, this research is designed to elucidate the relationship between the number of recovery strategies employed and the duration required for recovery from cyberbullying incidents. At the same time, victims’ evaluations of the effectiveness of various assistive strategies are collected.
Hypotheses:
H1: The longer the time spent experiencing cyberbullying, the longer it takes to recover.
H2: The fewer assistive strategies used, the longer the time required for recovery from cyberbullying.
H3: Utilising self-perceived effective assistive strategies is beneficial in shortening the recovery time.
3.Methodology
This study is designed to collect data on Chinese adolescents’ experiences with cyberbullying, the duration of recovery, and the implementation of support strategies through an online survey. In the survey, there are questions in terms of participants’ age, the number of cyberbullying experiences, the most impactful instance of cyberbullying, recovery time, adopted support strategies, and self-assessment of the effectiveness of these strategies [7].
3.1.Research Design
To obtain more precise, effective and specific data, the current study has been designed as a quantitative research investigation. To be specific, quantitative research focuses on measurable and computable data, which enables cyberbullying phenomena and trends to be objectively and accurately analysed [8]. By utilising statistical data and algorithms, researchers can quantify the duration of cyberbullying and the recovery time. Besides, this research method featured relatively enhanced visibility and persuasive power, which facilitates the exploration of the relationship between the number of support strategies and recovery time from cyberbullying. By relying on data and facts, quantitative research minimises researcher bias and enhances the objectivity and generalisability of the study. In the current research, the questionnaire adopted has a Cronbach’s alpha coefficient of 0.973, and a Kaiser-Meyer-Olkin (KMO) value of 0.915.
3.2.Participants
In this study, participants are individuals aged 18 and above, as they represent the primary user group of social media platforms and are considered to be responsible for their actions. Also, it is thought that they have better self-regulation abilities compared to minors when faced with retrospective questions that may evoke negative emotions. Participants voluntarily joined the study through a questionnaire link on social media, which is similar to Facebook named Weibo. A total of 103 questionnaires were collected, of which the male participation rate is 36.89% and the female participation rate is 63.11%.
3.3.Data Collection and Analysis
The data were processed using SPSS. Linear regression models were employed to measure the association between the duration of cyberbullying (independent variable) and the required recovery time (dependent variable); the number of adopted support strategies (independent variable) and the duration of negative emotion recovery (dependent variable); and self-perceived effectiveness of support strategies (independent variable) and recovery time from negative emotions (dependent variable). Through linear regression, the strength, direction, and significance of the relationships between two variables can be better examined.
3.4.Limitations and Ethical Considerations
In this study, the results can only represent Chinese user groups since the data collection was conducted exclusively through the Internet within China. The survey does not involve any questions related to personal privacy, nor does it record any contact information that could be linked to the participants. Moreover, all questionnaires were completed anonymously, and the data was used solely for this study.
4.Results
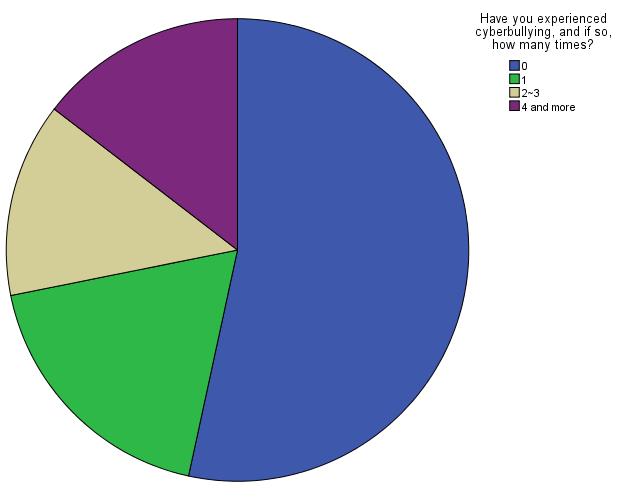
Figure 1: Frequency of cyberbullying incidences.
As can be seen from figure 1, it is suggested by close to half of those who have been subjected to cyberbullying that cyberbullying is a relatively common phenomenon and deserves to be studied in depth.
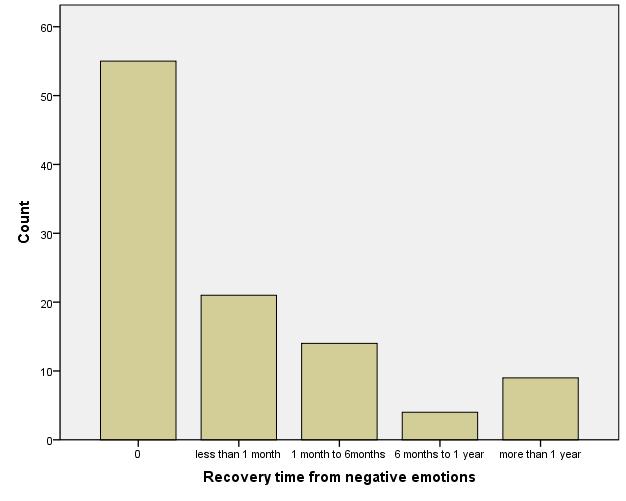
Figure 2: Duration of recovery from cyberbullying.
In figure 2, most recovery time is between 0 and 6 months, which shows that cyberbullying can exert a significant impact on a person’s mind and body and takes much time to recover.
Table 1: Selection instances of supportive strategies.
Support strategies |
Times |
Conveying feelings to family members |
12 |
Sharing emotions with friends |
40 |
Seeking assistance from psychological counseling institutions |
6 |
Seeking support from religious or faith-based sources |
2 |
Personal emotional venting |
27 |
Seeking the aid of cyber police |
4 |
Acceptance |
11 |
Evasion |
15 |
Clarification |
13 |
Counterattack |
14 |
According to Table 1, for the support strategies, talking to a friend was chosen most often at 40 times, followed by private emotional venting at 25 times, with the rest of the strategies chosen less than 20 times. This suggests that when faced with cyberbullying, people are more likely to seek out friends or self-digestion rather than resort to other strategies. Seeking help from religion or belief is the least frequent due to the relatively small number of people of religious faith in China. In addition, of all strategies at 4 times, seeking out the internet police is the second least chosen, which indicates that when encountering cyberbullying, many people do not choose to call the police to solve the problem and have no deep understanding of cyberbullying, and therefore there should be more measures to promote people’s awareness of cyberbullying.
Table 2: Self-assessment of the effectiveness level of supportive strategies.
Support strategies |
Average score |
Conveying feelings to family members |
2.33 |
Sharing emotions with friends |
4.23 |
Seeking assistance from psychological counseling institutions |
2.13 |
Seeking support from religious or faith-based sources |
1.71 |
Personal emotional venting |
3.58 |
Seeking the aid of cyber police |
1.98 |
Acceptance |
2.60 |
Evasion |
2.92 |
Clarification |
2.69 |
Counterattack |
3.23 |
From the perspective of support strategies, the highest mean feeling effectiveness score of 4.23 was for choosing to talk to a friend, which is consistent with the performance of the results mentioned above as shown in table 2. In other words, there is a greater proportion of people who chose to talk to their friends since they generally felt that talking to their friends played a more effective role in getting out of the predicament of being cyberbullied. Conversely, because Chinese people do not have a strong attachment to religion and faith, they do not choose to solve their problems through religion or faith when faced with cyberbullying. In addition, people may have no deep understanding of the role of the Internet police, nor do they recognise that cyberbullying is a cybercrime, and therefore they do not think it very effective to seek help from the Internet police.
To build a linear regression model, the duration of cyberbullying is taken as the independent variable and the required recovery time is used as the dependent variable. The ANOVA table obtained is shown below in table 3.
Table 3: ANOVA analysis of the duration of cyberbullying and recovery time.
| ANOVA | Model | Sum of Squares | df | Mean Square | F | P | Regression | 8.115 | 1 | 8.115 | 7.062 | .011 | Residual | 52.864 | 46 | 1.149 | Total | 60.979 | 47 |
Since ANOVA yields an F-test of 7.062 and p=0.011<0.05, the model plays a significant role and it makes sense to study the relationship between the duration of cyberbullying and time spent recovering. In the table below, the model-specific parameter estimates and test results are shown in table 4.
Table 4: Relationship between duration of cyberbullying and recovery time.
| Model | Coefficients | t | P | 95.0% Confidence Interval for B | B | Std. Error | Lower Bound | Upper Bound | (Constant) | 1.346 | .297 | 4.528 | .000 | .748 | 1.945 | X | .463 | .174 | 2.657 | .011 | .112 | .813 |
In the regression model, the regression parameter for the duration of cyberbullying is 0.463, which suggests a positive relationship between the duration of cyberbullying and the time of recovery. In addition, the t-test amount is 2.657, p=0.011<0.05 and the 95% confidence interval for the regression coefficient is [0.112, 0.813], which shows that the longer the duration of cyberbullying, the longer the recovery time, and that the relationship between the two is significant.
To build a linear regression model, the number of support strategies is adopted as the independent variable and the recovery time is taken as the dependent variable. The ANOVA table obtained is shown below in table 5.
Table 5: ANOVA analysis of the number of recovery strategies used and recovery time.
| ANOVAa | Model | Sum of Squares | df | Mean Square | F | P | Regression | 10.242 | 1 | 10.242 | 9.286 | .004 | Residual | 50.737 | 46 | 1.103 | Total | 60.979 | 47 |
ANOVA yields an F-test of 9.286 and p=0.004<0.05, and therefore the model is significant and it makes sense to study the relationship between the number of support strategies adopted and time spent recovering. The model specific parameter estimates and test results are shown in the table below in table 6.
Table 6: Relationship between the number of recovery strategies used and recovery time.
| Model | Coefficients | t | P | 95.0% Confidence Interval for B | B | Std. Error | Lower Bound | Upper Bound | (Constant) | .839 | .416 | 2.015 | .050 | .001 | 1.677 | X | .394 | .129 | 3.047 | .004 | .134 | .654 |
In the regression model, the regression parameter for the number of support strategies adopted is 0.394, which indicates a positive relationship between the number of support strategies adopted and the time of recovery. Besides, the t-test amount is 3.047, p=0.004<0.05 and the 95% confidence interval for the regression coefficient is [0.134, 0.654], which shows that the more the adopted number of support strategies requires a longer recovery time and that the relationship between the two is significant.
To build a linear regression model, the perceived degree of effectiveness of the strategy is taken as the independent variable and the required recovery time is used as the dependent variable. The ANOVA table obtained is shown below in table 7.
Table 7: ANOVA analysis of the self-assessed effectiveness of strategies and recovery time.
| ANOVAa | Model | Sum of Squares | df | Mean Square | F | P | Regression | 3.006 | 1 | 3.006 | 2.385 | .129b | Residual | 57.973 | 46 | 1.260 | Total | 60.979 | 47 |
NOVA yields an F-test of 2.385 and p=0.129, and hence the model is not significant. The model specific parameter estimates and test results are shown in the table 8 below.
Table 8: Relationship between the self-assessed effectiveness of strategies and recovery time.
| Model | Coefficients | t | P | 95.0% Confidence Interval for B | B | Std. Error | Lower Bound | Upper Bound | (Constant) | 2.747 | .497 | 5.523 | .000 | 1.746 | 3.748 | X | -.027 | .017 | -1.544 | .129 | -.061 | .008 |
In the regression model, the regression parameter for the perceived degree of effectiveness of the strategy is -0.027, which presents a negative relationship between the perceived degree of effectiveness of the strategy and the time of recovery. Besides, the t-test amount is -1.544, p=0.129 and the 95% confidence interval for the regression coefficient is [-0.061, 0.008], which indicates that the greater the perceived degree of effectiveness of the strategy, the less recovery time is required.
Cyberbullying is considered a common phenomenon in daily life, and though bullying does not last very long, a good deal of time is taken to recover from it. The recovery time is closely related to the duration of cyberbullying, the number of support strategies adopted and the perceived degree of effectiveness of the strategy. In particular, there is a positive correlation between recovery time and the duration of cyberbullying and the number of support strategies adopted and a negative correlation between recovery time and the perceived degree of effectiveness of the strategy. Therefore, both of them play a crucial role if the problem of cyberbullying is to be better addressed.
5.Discussion
The results of this study align with Hypotheses 1 and 3, while not supporting Hypothesis 2.
First of all, in consistency with most trauma responses, the results show that extended cyberbullying exposure correlates with a prolonged recovery period. This is akin to the detrimental impacts of chronic stress on human health as described by McEwen’s concept of “allostatic load” [9]. Often, bullying victims face high levels of chronic stress, which can lead to long-term effects, including various psychopathologies in adulthood [10]. This supports the idea that enduring bullying can result in substantial recovery periods. Through escalating allostatic load, excessive chronic stress can trigger stress mediators’ damaging effects [9]. Bullying, especially when persistent, equates to psychological trauma. Copeland et al. proposed a higher risk of mental health issues in adults bullied as children, a risk that persists even after accounting for pre-existing psychiatric issues and family hardships [11]. Accordingly, it is suggested that cyberbullying is a form of chronic stressor that exposes victims to trauma for prolonged and unpredictable periods. Therefore, the finding, which indicates that the longer the duration of exposure to cyberbullying, the longer the recovery time required, conforms to the negative impacts observed in other forms of bullying.
Hypothesis 2 is not supported, possibly due to therapeutic dependency and repeated revisiting of trauma when receiving various therapeutic strategies. Therapeutic dependency often occurs when a patient relies heavily on the therapist for support. In therapeutic approaches that cultivate strong therapeutic relationships, there may be a particularly high risk of dependency. Freud and colleagues discussed strong therapist-patient relationships may cause dependency and prolong therapy [12]. However, dependency is not necessarily negative since it may represent a stage in the therapeutic process where the client learns to rely on others. If improperly improperly managed, it may hinder the therapeutic process as the patient may resist progress towards autonomy.
A robust therapeutic alliance is crucial in therapy, particularly when working with victims of bullying or trauma. Martin, Garske and Davis found that a strong therapeutic alliance was reliable for positive therapeutic outcomes across therapy and patient populations [13]. Bucci et al. proposed that a stronger therapeutic alliance was associated with better outcomes [14]. In this therapeutic model, therapists should regularly reassess the balance between therapeutic alliance and dependency [15]. In addition to therapeutic dependency, victims of cyberbullying seeking help in various forms may need to repeatedly recount their traumatic experiences due to different support providers, potentially prolonging recovery time.
Repeatedly recounting traumatic experiences when seeking help for psychological issues may prolong the time to overcome trauma. Briere and Scott proposed excessive or uncontrolled revisiting of trauma may cause retraumatisation, potentially lengthening recovery time, which requires a balance between exposure and potential for retraumatisation [16]. Ehlers and Clark found dysfunctional coping strategies maintain PTSD symptoms [17]. However, Foa, Hembree, and Rothbaum discussed that avoiding traumatic memories prevent the individual from processing the trauma in a therapeutic context, thereby prolonging distress [18]. With no one-size-fits-all approach in trauma therapy, the impact of individual differences in selecting assistance strategies for cyberbullying needs further investigation.
In the negative correlation between recovery time and perceived strategy effectiveness, it is suggested that higher self-perceived effectiveness of auxiliary strategies leads to shorter recovery times. By introducing five key recovery processes (“CHIME”), Leamy et al. asserted that an individual’s view of their treatment significantly affects these processes, particularly empowerment [19]. This might be the reason why “seeking help from friends” has emerged as the most popular and effective strategy. Often, patient involvement in their treatment strategy enhances outcomes and empowerment. Similarly, a systematic review found that patients who viewed their treatment as effective were more likely to engage in treatment and attain better health outcomes, which supports the self-determination theory [20, 21].
However, though these self-perceived strategies may play a beneficial role, they cannot substitute evidence-based treatment, as patient perceptions may be influenced by personal biases or misinformation and may not align with proven treatments [22]. Therefore, to enhance positive patient perceptions of their treatment, an ideal support approach for cyberbullying’s aftermath might combine professional mental health care with strategies.
6.Conclusion
In conclusion, this research contributed to the field of cyberbullying as it underscored the impact of duration of exposure, therapeutic dependency and perceived strategy effectiveness on recovery time. As to other forms of bullying, the chronic stress and long-lasting negative effects of cyberbullying were reaffirmed. A potential issue of therapeutic dependency prolonging the recovery process is stressed, and the critical balance between dependency and therapeutic alliance is highlighted. Also, revisiting traumatic experiences repeatedly potentially delays recovery despite its benefits in certain therapeutic contexts [18]. This result emphasises the necessity of tailoring therapy to individual needs and responses. Furthermore, the inverse correlation between recovery time and perceived strategy effectiveness informs how victims’ perceptions might influence recovery [22].
The limitations inform future research. Further investigations should encompass more diverse populations since cyberbullying affects different age groups. In addition, the knowledge base on cyberbullying recovery is further enriched by probing deeper into why adopting multiple strategies might extend recovery and how various strategies provide a perception of effectiveness. The participant pool, mainly Chinese university students, may not generalise the situation, and thus future research should collect samples from varied regions and consider cyberbullying among underage victims. Employing multiple auxiliary strategies might extend the recovery period from cyberbullying, suggesting further study into the effects of different recovery strategies. Lastly, with possible variations of the perception of the effectiveness of auxiliary strategies among victims, future research should focus on identifying aspects contributing to the perception of “effectiveness” for each strategy.
A more nuanced understanding of cyberbullying recovery is enabled. They highlight the need for personalised and evidence-based approaches to therapy and incorporating patient perspectives into treatment plans. Through informing the development of more effective strategies to support victims of cyberbullying, this research benefits the recovery and wellbeing of individuals affected by this pervasive issue.
References
[1]. Belsey, B. (2005). Cyberbullying: An emerging threat to the always on generation. http://cyberbullying.ca/pdf/feature_dec2005.pdf
[2]. Steeves, V. (2005). Young Canadians in a wired world, phase II: Trends and recommendations. Media Awareness Network. http://www.mediaawareness.ca/english/research/YCWW/phaseII/upload/YCWWII_student_survey.pdf
[3]. Ybarra, M. L., Mitchell, K. J., Wolak, J., & Finkelhor, D. (2006). Examining characteristics and associated distress related to Internet harassment: Findings from the second Youth Internet Survey. Paediatrics, 118:1169-1177.
[4]. Ridout, B., & Campbell, A. (2018). The use of social networking sites in mental health interventions for young people: Systematic review. J Med Internet Res, 20(12), e12244.
[5]. Hellfeldt, K., López-Romero, L., & Andershed, H. (2019). Cyberbullying and psychological well-being in young adolescence: The potential protective mediation effects of social support from family, friends, and teachers. Int J Environ Res Public Health, 17(1).
[6]. Juvonen, J., & Gross, E. F. (2008). Extending the School Grounds?-Bullying Experiences in Cyberspace. Journal of School Health, 78(9), 496–505.
[7]. Hu, Q., Bernardo, A. B. I., Lam, S. W., & Cheang, P. K. (2018). Individualism-Collectivism Orientations and Coping Styles of Cyberbullying Victims in Chinese Culture. Current Psychology, 37(1): 65–72.
[8]. Opdenakker, R. (2006). Advantages and disadvantages of four interview techniques in qualitative research. Forum Qualitative Social Research, 7(4):10.
[9]. McEwen B. S. (1998). Protective and damaging effects of stress mediators. The New England Journal of Medicine, 338(3): 171–179.
[10]. Klomek, A. B., Sourander, A., & Elonheimo, H. (2015). Bullying by peers in childhood and effects on psychopathology, suicidality, and criminality in adulthood. The Lancet. Psychiatry, 2(10): 930–941.
[11]. Copeland, W. E., Wolke, D., Angold, A., & Costello, E. J. (2013). Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA psychiatry, 70(4): 419–426.
[12]. Freud, S. (2001). The standard edition of the complete psychological works of Sigmund Freud. Random House, London.
[13]. Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance with outcome and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychology, 68(3):438–450.
[14]. Bucci, S., Berry, K., Barrowclough, C., & Haddock, G. (2016). Family interventions in psychosis: A review of the evidence and barriers to implementation. Australian Psychologist, 51(1): 62-68.
[15]. Horvath, A. O., Del Re, A. C., Flückiger, C., & Symonds, D. (2011). Alliance in individual psychotherapy. Psychotherapy (Chicago, Ill.), 48(1): 9–16.
[16]. Briere, J. N., & Scott, C. (2015). Principles of trauma therapy: A guide to symptoms, evaluation, and treatment (2nd ed., DSM-5 update). Sage Publications, Inc.
[17]. Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4): 319–345.
[18]. Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences: Therapist guide. Oxford University Press.
[19]. Leamy, M., Bird, V., Boutillier, C. L., Williams, J., & Slade, M. (2011). Conceptual Framework for personal recovery in Mental Health: Systematic Review and narrative synthesis. British Journal of Psychiatry, 199(6):445–452.
[20]. Kukla, M., Salyers, M. P., & Lysaker, P. H. (2013). Levels of patient activation among adults with schizophrenia. Journal of Nervous & Mental Disease, 201(4): 339–344.
[21]. Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1): 68–78.
[22]. Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.). Routledge/Taylor & Francis Group.
Cite this article
JIANG,X. (2023). The Relationship Between the Length of Recovery from Cyberbullying and the Number of Assistive Strategies Employed by Victims and the Quality of Self-perceived Assistive Strategies. Communications in Humanities Research,11,1-10.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Educational Innovation and Philosophical Inquiries
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Belsey, B. (2005). Cyberbullying: An emerging threat to the always on generation. http://cyberbullying.ca/pdf/feature_dec2005.pdf
[2]. Steeves, V. (2005). Young Canadians in a wired world, phase II: Trends and recommendations. Media Awareness Network. http://www.mediaawareness.ca/english/research/YCWW/phaseII/upload/YCWWII_student_survey.pdf
[3]. Ybarra, M. L., Mitchell, K. J., Wolak, J., & Finkelhor, D. (2006). Examining characteristics and associated distress related to Internet harassment: Findings from the second Youth Internet Survey. Paediatrics, 118:1169-1177.
[4]. Ridout, B., & Campbell, A. (2018). The use of social networking sites in mental health interventions for young people: Systematic review. J Med Internet Res, 20(12), e12244.
[5]. Hellfeldt, K., López-Romero, L., & Andershed, H. (2019). Cyberbullying and psychological well-being in young adolescence: The potential protective mediation effects of social support from family, friends, and teachers. Int J Environ Res Public Health, 17(1).
[6]. Juvonen, J., & Gross, E. F. (2008). Extending the School Grounds?-Bullying Experiences in Cyberspace. Journal of School Health, 78(9), 496–505.
[7]. Hu, Q., Bernardo, A. B. I., Lam, S. W., & Cheang, P. K. (2018). Individualism-Collectivism Orientations and Coping Styles of Cyberbullying Victims in Chinese Culture. Current Psychology, 37(1): 65–72.
[8]. Opdenakker, R. (2006). Advantages and disadvantages of four interview techniques in qualitative research. Forum Qualitative Social Research, 7(4):10.
[9]. McEwen B. S. (1998). Protective and damaging effects of stress mediators. The New England Journal of Medicine, 338(3): 171–179.
[10]. Klomek, A. B., Sourander, A., & Elonheimo, H. (2015). Bullying by peers in childhood and effects on psychopathology, suicidality, and criminality in adulthood. The Lancet. Psychiatry, 2(10): 930–941.
[11]. Copeland, W. E., Wolke, D., Angold, A., & Costello, E. J. (2013). Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA psychiatry, 70(4): 419–426.
[12]. Freud, S. (2001). The standard edition of the complete psychological works of Sigmund Freud. Random House, London.
[13]. Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance with outcome and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychology, 68(3):438–450.
[14]. Bucci, S., Berry, K., Barrowclough, C., & Haddock, G. (2016). Family interventions in psychosis: A review of the evidence and barriers to implementation. Australian Psychologist, 51(1): 62-68.
[15]. Horvath, A. O., Del Re, A. C., Flückiger, C., & Symonds, D. (2011). Alliance in individual psychotherapy. Psychotherapy (Chicago, Ill.), 48(1): 9–16.
[16]. Briere, J. N., & Scott, C. (2015). Principles of trauma therapy: A guide to symptoms, evaluation, and treatment (2nd ed., DSM-5 update). Sage Publications, Inc.
[17]. Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4): 319–345.
[18]. Foa, E. B., Hembree, E. A., & Rothbaum, B. O. (2007). Prolonged exposure therapy for PTSD: Emotional processing of traumatic experiences: Therapist guide. Oxford University Press.
[19]. Leamy, M., Bird, V., Boutillier, C. L., Williams, J., & Slade, M. (2011). Conceptual Framework for personal recovery in Mental Health: Systematic Review and narrative synthesis. British Journal of Psychiatry, 199(6):445–452.
[20]. Kukla, M., Salyers, M. P., & Lysaker, P. H. (2013). Levels of patient activation among adults with schizophrenia. Journal of Nervous & Mental Disease, 201(4): 339–344.
[21]. Ryan, R. M., & Deci, E. L. (2000). Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. American Psychologist, 55(1): 68–78.
[22]. Wampold, B. E., & Imel, Z. E. (2015). The great psychotherapy debate: The evidence for what makes psychotherapy work (2nd ed.). Routledge/Taylor & Francis Group.