






1. Introduction
Humans are highly social and visual creatures. Therefore, facial appearance plays a vital role in our daily social life. Previous research shows that facial affect recognition is the bedrock of successful social interaction [1]. As we all know, facial appearance can reflect much information about a person.
From the previous research, we can find that as minimal an exposure time as a tenth of a second is sufficient for people to make a specific trait inference from facial appearance [2]. Moreover, another research shows that naive perceivers can read sexual orientation from other individuals' unknown faces [3]. Many other things that seem weak in correlation with facial appearance are linked. So, we are considering whether we can learn more from facial appearances.
Reliable, fact-proved, scientifically studied, up-to-date estimates of the proportion of a general population affected by different diseases or health conditions are essential to effective health policy, planning, and evaluation [4]. Not everyone’s health condition, primarily mental, can be easily seen or identified by their appearance or appearance. Personality disorders, mood disorders, and mental diseases often require long-term observations and thorough medical examination [5]. However, it is hard to hide happy emotions and pain; what can be accurately guessed through our facial expressions and countenance is discomfort, ill-at-easiness, anxiety, depression, and torture. Sleeplessness, insomnia, destructive appetite, restlessness, and fear may directly show the mental condition.
Epidemiological studies of the prevalence and incidence of a range of psychiatric disorders have now been undertaken in a wide range of low-, middle- and high-income countries, which have contributed significantly to a better understanding of how common various mood disorders, personality disorders and unhealthy state of mind are across the world. Advances in measuring the fatal and non-fatal consequences of these diseases – including quantification of time spent in a state of ill health – have also enabled a more systematic comparison of the relative contribution that different diseases and their underlying risk factors make to the overall toll of death and disability [6]. In addition, more research is done on the relationship between mental health conditions and facial expressions that provide the latest available estimates of the prevalence of depression and other common mental disorders at the global and regional level, together with data concerning the consequences of these disorders in terms of lost health [7].
Country-specific estimates provided by various health-related organizations to help control and prevent fatal consequences offer complementary information to those provided in other information products developed by WHO and others on the appropriate public health response to these disorders, including their treatment and prevention (http://www.who.int/topics/depression, http://www.who.int/mental_health/mhgap). Common mental disorders refer to two main diagnostic categories: depression and anxiety. In addition, more and more studies on appearances and facial expressions are conducted to better judge and evaluate the changeable health conditions and emotions in different life situations [8].
From the previous research, trait neuroticism is associated with several mental health vulnerabilities [9] and is highly correlated with a general factor for psychopathology [10]. Moreover, we also can prove that people can judge others' personalities through facial appearances [11]. This research shows how mental health can be related to one's personality and can be judged by facial appearance. To go deeper into the relationship, some researchers have been conducted into the ability to recognize clinically related conditions from facial images [12]. Moreover, some researches show that facial appearance can hold cues for symptoms of depression [13]. That means at least one mental illness can be seen through facial appearances. Another research shows that perceived mental health reflects actual mental health [14]. This research has proved another point of the relationship between mental illness and judgments.
Previous research has drawn some conclusions to prove that depression is visible. However, little research discusses the relationship between facial appearances and other mood disorders or personality disorders. Moreover, the accuracy of the judgments of these disorders is not being shown yet.
So, our research will mention three hypotheses about the questions mentioned above.
2. Hypotheses
Hypothesis 1. Mental health condition (e.g., healthy state of mind, mood disorders, personality disorders) can be accurately judged under facial appearance.
Hypothesis 2. Mood disorders (e.g., depression, anxiety) are more visible than personality disorders (e.g., borderline personality disorder, histrionic personality disorder).
Hypothesis 3. People with mood disorders can judge faces under the same conditions more accurately.
3. Method
Experiment 1
Can mental health conditions be accurately judged by facial appearance? For example, are mood disorders more visible than personality disorders?
3.1. Participants
Our experiment will cooperate with hospitals and medical institutions. One hundred eighty individuals will be recruited to provide photos of their faces in exchange for 50 yuan. 40% will be under healthy mental conditions, 30% will be under mood disorders (e.g., depression, anxiety), and we will use the HAD to measure the severity of their mood disorders. 30% of them will be under personality disorders (e.g., borderline personality disorder, histrionic personality disorder), and we will use the MMPI to measure the severity of their personality disorders. The individuals need to sign agreements in case of ethical problems.
Our primary hypothesis involved assessing the accurate mental health data according to facial appearances. We performed a power analysis using the software package G*Power (Erdfelder, Faul, & Buchner, 1996). The results indicated that with N=134, our experiment could detect an effect size of Cohen’s d of 0.3, using a paired t-test at a 5% alpha level (two-tailed) threshold with 80% statistical power.
Our secondary hypothesis involved assessing the comparison between the accuracy of judgments on mood disorders and personality disorders. We performed a power analysis using the software package G*Power (Erdfelder, Faul, & Buchner, 1996). The results indicated that with N=134, our experiment could detect an effect size of Cohen’s d of 0.3, using a z-score to standardize the observers' HAD, MMPI, and health scores.
3.2. Experimental Design
We will use a quasi-experimental design.
3.3. Procedures
Observers will be shown random pictures of the facial appearance and use
the 7-point Likert scale to rate the questions below:
How healthy do you think he/she is? (1 means very unhealthy--------- 7 is very healthy)
How do you think his/her sleep quality is? (7 means very good--------- 1 means very bad)
Do you think he/she could complete a task on time? (1 means very--------- 7 means absolutely not)
Does he/she often quit? (1 means very-------- 7 means absolutely not)
How likable do you think he/she is? (7 means very---------1 means absolutely not)
The total score will be 35, and the higher score represents that the face is judged to be healthier, and the lower score represents that the face is judged to be unhealthier.
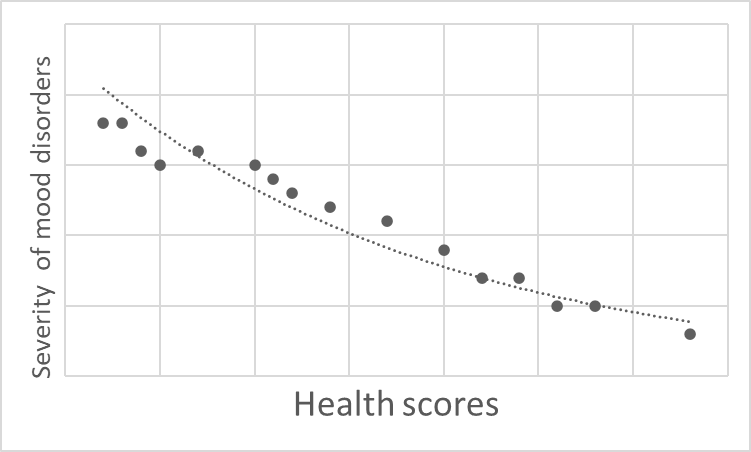
Figure 1: Shows the scatter plots of mood disorders.
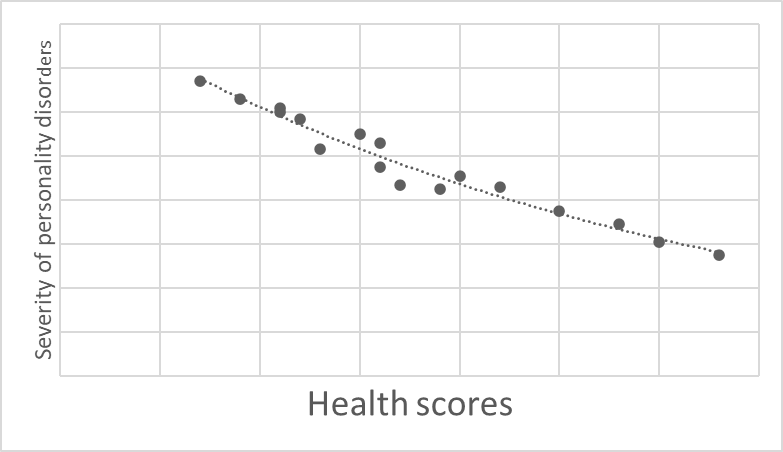
Figure 2: Shows the scatter plots of personality disorders.
3.4. Data Analytic Approach
We will use scatter plots to measure the correlation between the severity of mood disorders and health scores. We will also measure the correlation between the severity of personality disorders and health scores. We separate mood disorders and personality disorders into two figures because the HAD and the MMPI use different measurements and ranges.
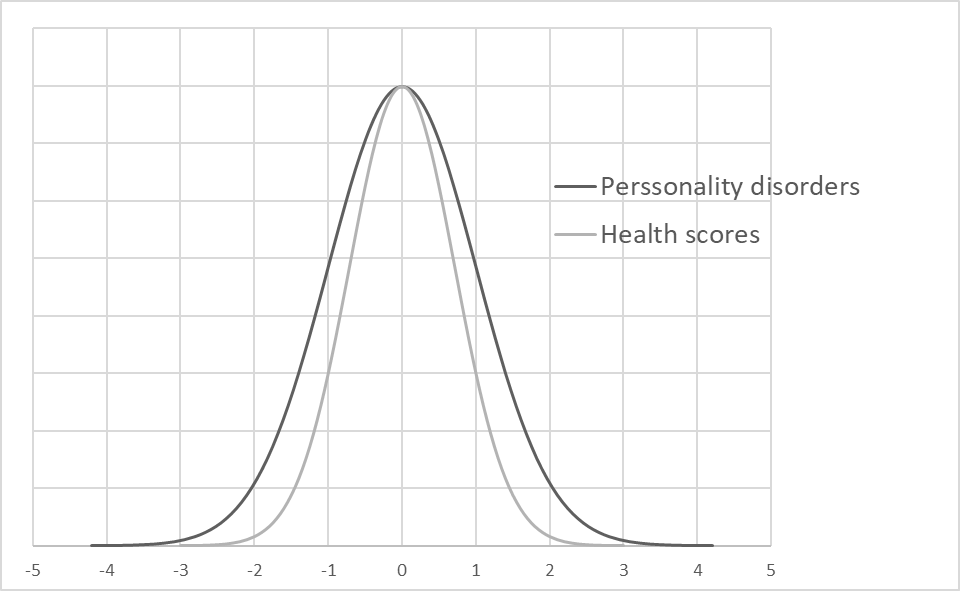
Figure 3: Measures the correlation between the severity of personality disorders and health scores.
Figure 4: The scatter plots to measure the correlation between the severity of mood disorders and health scores.
3.5. Data Analytic Approach
Because HIV and MMPI have different measurements and ranges, so we will use the z-score to standardize our data. For example, we will combine the severity of mood disorders with health scores and put them into one figure. We will also combine the severity of personality disorders and health scores into another figure. The closer the scores of the scales are, the more data coincide, and the more accurate the result is.
4. Results
Aim 1. As illustrated in Figure 1 and Figure 2, we predict that there will be a negative correlation between the severity of disorders and health scores. So, it could prove our first hypothesis that mental health can be accurately judged by observing facial appearances.
Aim 2. As illustrated in Figure 3 and Figure 4, we predict that the severity of mood disorders has more proximity data with health scores. So, it can prove our second hypothesis that mood disorders are more visible than personality disorders.
4.1. Experiment 2
Can people with mood disorders judge faces under the same conditions more accurately?
Method
Participants. We will use the same photos of faces that are used in Experiment 1
Our tertiary hypothesis involves assessing the accuracy of people's judgments under mood disorders. We performed a power analysis using the software package G*Power (Erdfelder, Faul, & Buchner, 1996). The results indicated that with N=325, our experiment could detect an effect size of Cohen’s d of 0.18 using ANOVA.
In order to find out whether people with mood disorders can be more accurate in judging faces under the same conditions, we will separate those 325 observers into three condition categories. About 40% of the participants are healthy, about 30% are under depression, and another 30% are under anxiety.
Experimental design. We will use the between-subject experimental design.
Procedures. Observers will be randomly separated into different computer rooms and complete the same question from Experiment 1
Figure 5: Shows the prediction that people with depression.
Data Analytic Approach. We will use the absolute value of the differences between the severity of disorders and health scores and compare the differences under different mental conditions. The lower the differences are, the more accurate the judgments are.
Results
Aim 1. As illustrated in Figure 5, we predict that people under depression can be more accurate in judging the faces under depression. In contrast, people from the anxiety group can be more accurate in judging the faces of anxiety.
5. General Discussion
As we mentioned before, mental health is essential to all of us. However, in our country, scant attention has been paid to mental disorders. We expect to find relationships between mental disorders and facial appearances. We hope that this research can improve the awareness of mental disorders. We also hope that we can offer intervention and treatment to those who have not realized they are under mental disorders.
There are also some limitations. Because the experiment will be conducted in China, while the facial appearances of different ethnic groups can be very different, we are questioning whether these conclusions can be changed across different ethnic groups, genders, and ages.
Moreover, for further research, we hope to find what specific facial features and indicators influence people's judgments of mental health conditions.
The data and the materials will be available on the Open Science Framework database.
References
[1]. Erickson K, Schulkin J. (2003) Facial expressions of emotion: a cognitive neuroscience perspective. Brain and Cognition, 52(1): 52-60.
[2]. Janine Willis, Alexander Todorov. (2006) First impressions: making up your mind after a 100-ms exposure to a face. Psychological Science, 17(7): 592-598.
[3]. Joshua A. Tabak, Vivian Zayas. (2012) The Roles of Featural and Configural Face Processing in Snap Judgments of Sexual Orientation. https://doi.org/10.1371/journal.pone.0036671
[4]. Üstün TN, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJL. (2004) Global burden of depressive disorders in the year 2000. British Journal of Psychiatry, 184: 386-392.
[5]. Baxter A, Scott JM, Vos T, Whiteford H. (2013) Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychological Medicine, 43: 897–910.
[6]. Ferrari A, Somerville AJ, Baxter A, Norman R, Patten S, Vos T, Whiteford H. (2013) Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychological Medicine, 43: 471–481.
[7]. Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, Vos T, Whiteford HA. (2013) Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. https://doi.org/10.1371/journal.pmed.1001547
[8]. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (2016) Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990-2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet, 388: 1545-1602.
[9]. Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010) Linking “Big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136(5): 768–821.
[10]. Caspi, A., Houts, R. M., Belsky, D. W., Goldman-Mellor, S. J., Harrington, H., Israel, S., … Moffitt, T. E. (2014) The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2(2): 119–137.
[11]. J Nonverbal Behav. (2014) Personality at Face Value: Facial Appearance Predicts Self and Other Personality Judgments among Strangers and Spouses. Journal of Nonverbal Behavior, 38: 259–277.
[12]. Shevlin, M., Walker, S., Davies, M.N.O., Banyard, P., Lewis, A.C.(2003)Can you judge a book by its cover? Evidence of self-stranger agreement on personality at zeroacquaintance. Personality and Individual Differences, 35 (6): 1373–1383.
[13]. Scott, N.J., et al. (2013) Facial cues to depressive symptoms and their associated personality attributions. Psychiatry Research. http://dx.doi.org/10.1016/j.psychres.2013.02.027
[14]. Robert Ward Naomi Jane Scott (2018) Cues to mental health from men’s facial appearance. https://doi.org/10.1016/j.jrp.2018.04.007
Cite this article
Wang,Y. (2023). Mental health condition can be seen through facial appearances. Advances in Economics, Management and Political Sciences,15,40-45.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Business and Policy Studies
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Erickson K, Schulkin J. (2003) Facial expressions of emotion: a cognitive neuroscience perspective. Brain and Cognition, 52(1): 52-60.
[2]. Janine Willis, Alexander Todorov. (2006) First impressions: making up your mind after a 100-ms exposure to a face. Psychological Science, 17(7): 592-598.
[3]. Joshua A. Tabak, Vivian Zayas. (2012) The Roles of Featural and Configural Face Processing in Snap Judgments of Sexual Orientation. https://doi.org/10.1371/journal.pone.0036671
[4]. Üstün TN, Ayuso-Mateos JL, Chatterji S, Mathers C, Murray CJL. (2004) Global burden of depressive disorders in the year 2000. British Journal of Psychiatry, 184: 386-392.
[5]. Baxter A, Scott JM, Vos T, Whiteford H. (2013) Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychological Medicine, 43: 897–910.
[6]. Ferrari A, Somerville AJ, Baxter A, Norman R, Patten S, Vos T, Whiteford H. (2013) Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychological Medicine, 43: 471–481.
[7]. Ferrari AJ, Charlson FJ, Norman RE, Patten SB, Freedman G, Murray CJ, Vos T, Whiteford HA. (2013) Burden of depressive disorders by country, sex, age, and year: findings from the global burden of disease study 2010. https://doi.org/10.1371/journal.pmed.1001547
[8]. GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (2016) Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 310 Diseases and Injuries, 1990-2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet, 388: 1545-1602.
[9]. Kotov, R., Gamez, W., Schmidt, F., & Watson, D. (2010) Linking “Big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin, 136(5): 768–821.
[10]. Caspi, A., Houts, R. M., Belsky, D. W., Goldman-Mellor, S. J., Harrington, H., Israel, S., … Moffitt, T. E. (2014) The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2(2): 119–137.
[11]. J Nonverbal Behav. (2014) Personality at Face Value: Facial Appearance Predicts Self and Other Personality Judgments among Strangers and Spouses. Journal of Nonverbal Behavior, 38: 259–277.
[12]. Shevlin, M., Walker, S., Davies, M.N.O., Banyard, P., Lewis, A.C.(2003)Can you judge a book by its cover? Evidence of self-stranger agreement on personality at zeroacquaintance. Personality and Individual Differences, 35 (6): 1373–1383.
[13]. Scott, N.J., et al. (2013) Facial cues to depressive symptoms and their associated personality attributions. Psychiatry Research. http://dx.doi.org/10.1016/j.psychres.2013.02.027
[14]. Robert Ward Naomi Jane Scott (2018) Cues to mental health from men’s facial appearance. https://doi.org/10.1016/j.jrp.2018.04.007