






1. Introduction
Autism Spectrum Disorder (ASD) is diagnosed based on two criteria, social communication and interpersonal interaction disorders, and repetitive behaviours and narrow interests, while delayed language development is one of the main reasons or features for the initial diagnosis [1-2]. The development of social communication functions is influenced by early motor skills related to language acquisition, and children with autism consistently show impairments in basic and complex motor skills that are closely associated with delayed or regressive speech development and social challenges [3]. According to the most recent evaluation of the study, PECS is considered a promising communication intervention for children with autism [4]. This is because images are easier to understand and do not require prerequisite skills such as eye contact and oral-motor skills, whereas Manual signs often require eye contact and mimicry, both of which are difficult for children with autism to acquire [1,5]. Furthermore, Although the visual-gestural model of sign language differs from the vocal-auditory model of language in several key aspects, deaf or severely autistic children with autism do exhibit sign language imitation and response, which provides new clues for analysing the purpose and functional understanding of the response in children with autism [6-7]. Therefore, this study attempts to use sign language to assist children with autism in describing a situation. The theoretical significance of this study lies in providing a referential theoretical framework for sign language intervention strategies concerning children with autism. While enhancing the ability of children with autism to describe situations and language development, it helps them integrate smoothly into mainstream educational institutions and the wider social structures, thereby increasing their sense of belonging and overall well-being.
2. Literature review
Children with severe autism can acquire communication skills through sign language and a combination of spoken and signed modalities [7]. Sign language and spoken language share similar phonology, morphology, and syntax, despite significant grammatical differences [8]. Currently, the AAC technical intervention for autistic children has shifted from sign language to a combination of pictures, symbols, and speech output from specialized devices [1]. Despite the limitations of sign language, it enhances the language quality of the participating groups. Therefore, attention should still be paid to sign language intervention for autistic patients to promote the diversification of intervention strategies [1]. Sign language is an effective means of enhancing communication for many people with non-verbal developmental disabilities. Visual cues are formed through the styling of symbols in sign language, and their figurative nature helps to transfer them to life situations, thus facilitating language learning [5]. Sign language is a language similar in structure to spoken language, having many of the attributes of spoken language, and sign language is closer to the use of spoken language than gestures [8]. Both sign language and spoken language involve phonological and syntactic processing areas in Broca's area, and Broca's area and its neighbouring cortex (Brodmann's area 45/47) are activated when there is an increased load of integrating gesture and speech in the language environment [9]. Broca's area, which is typically associated with internal language processing, also integrated for movement observation and speech. This demonstrates that language and movement processing share a high-level neurological integration system [9]. Research has confirmed that in most speech-gesture pairs, the strokes are consistent with the corresponding speech fragment, which may be a single word or phrase [10].
3. Research design and implementation
3.1. Study subjects
The subject of this study was a 7-year-old child who was diagnosed with ASD with speech disorder by professional assessment of a hospital physician and met the DSM-5 classification criteria in the Support Needs Category (Mild Disorder). The researcher interviewed the rehabilitation teachers and kindergarten teachers of the special institution about the subject's intervention, and after collecting their opinions or feedbacks, a summary table of the study subject's competencies was compiled. Subject has good mimicry skills, including large movements and a few fine movements. Engagement in learning is largely dependent on the presentation of the learning material. The visual material can maintain for a longer period of time (about 45mins-1h). Otherwise, problematic behaviours such as loud talking, crying, etc. will occur frequently. In terms of social skills, the subject had speech impairment. Frequently used nouns (e.g., cake, etc.) and actions (e.g., pushing others, etc.) in isolation to express meaning. Inability to express needs or answer questions use complete sentences. When asked to describe "who/what + what" or "who/what + where + what" in real scenes, picture books or pictures, the subject could only answer using nouns or verbs alone, such as "what/who" and "what". Adjectives, prepositions, and quantifiers are never involved, and only when asked individually are responses given truthfully, but with a low rate of accuracy. Nouns and verbs were the best mastered, followed by adjectives and quantifiers, and prepositions were the worst mastered.
3.2. Related work
This study adopted the A-B-M design of the single-subject research method. A denotes the baseline period, B denotes the intervention period, and M denotes the maintenance phase after the intervention withdrawal. In the baseline period, there was no teaching and the intervener tested the subject on both short and long sentence expressions. The data collection in the baseline period consisted of six data points and was conducted in three sessions (three days) of 20 minutes each. The intervention period is the intervention in sign language teaching, in which the learning of sign language movements is based on discrete trial teaching (DTT), the training of sign language-assisted oral expression is based on verbal behavior (VB) teaching, where the teaching is controlled by the intra-verbal of the linguistic stimuli. The training was based on the graded training system teaching strategy, which subdivided the teaching skills into acceptable ranges for the subject and followed the principle of “decreasing prompts” to enable the subject to realize learning autonomy [11]. The test was divided into the mastery of sign language action (at least 3 consecutive points pass rate of 80% or more), and the contextual description post-test (at least 3 consecutive points pass rate of 80% or more) [12]. The intervention training tool features standardized sign language from "Chinese Sign Language Teaching," focusing on prepositions, verbs, adjectives, and quantifiers. To prevent the 'practice effect' that could bias results, situational pictures from children's books were used as assessment tools during the intervention while story situation pictures developed by the researchers were used during the baseline and maintenance phases. In addition, the subject was taught sign language with the palms and fingers oriented in the opposite direction of the correct direction so that he/she could learn the correct sign language [6]. The maintenance period is a test administered one week after the end of the intervention period to observe and collect test data for pre- and post-intervention comparisons. The subject's ability to describe a situation through auxiliary aids was measured, with a minimum of 3 points collected during the maintenance period and no passing or failing criteria.
3.3. Variables
The independent variable in this study were the auxiliary sign language intervention programme. Dependent variable is the effectiveness of sign language in assisting spoken language in its ability to describe a situation. One point is awarded for each correct word, and no points are given for unrelated, grammatical, or incorrect words, and the data are used to measure the correctness of the subject's independent responses. The control variables were divided into four components, the instructor, the assessment method, the location of the intervention experiment and the assessment, and the data recorders.
4. Result
4.1. Inter-observer reliability
The formula for calculating the percentage of inter-observer reliability is: inter-observer reliability=number of times of consistency/(number of times of consistency+number of times of inconsistency)×100%, and the reliability index should preferably be between 80% and 100% [12]. In this study, it was calculated that both Recorder A and Recorder B had a test-observation concordance of more than 85% regarding the study participants. Whether the participants were able to describe the picture situation through sign language during the test, the observational agreement between the two recorders reached 100% at baseline, 95.5% at intervention, and 98.5% at maintenance. As the inter-observer agreement at all stages was above 85%, it indicated a certain degree of confidence in the observation.
4.2. C-statistical analyses
4.2.1. Immediate effectiveness
As depicted in Figure 1 and Table 1, during the baseline period, the full range of the level is 2-2, the change in the level during the period is 0, and the average level is 2. This indicates a stable and isochronous trend, with both level and trend stability at 100%. Given the stable and unimproving trend observed in the baseline period, the intervention period was initiated. Since all data points in the baseline period are the identical, it is not appropriate to calculate the C-value [12].
Upon entering the intervention period, the full distance of the level is 4-5, with a change in level within the phase of 1, and the average level of 4.5. This also represents a stable trend, with both level and trend stability at 100%. According to the results of the C-statistics, the C-value for the intervention period was -0.125 and the Z-value was 0.23, which did not meet the 0.05 criterion of significance, indicating no significant difference and a stable, non-significant change in the trend.
When comparing the baseline period to the intervention period, the change in level between phases was 3, the change in average level was 2.5, and there was a change in the trend direction of the outcome. The trend stability changed from stable to stable, with 0 percent overlap. Although there was no change in the interphase trend and outcome between the baseline and intervention periods, the average level in the intervention period was higher than that in the baseline period. According to the results of the within-stage C-statistics, the C-value is 0.71 and the Z-value is 3.55, reaching a significant level of 0.01, which is a significant difference. Therefore, there is a significant positive intervention effect and a trend towards significant change.
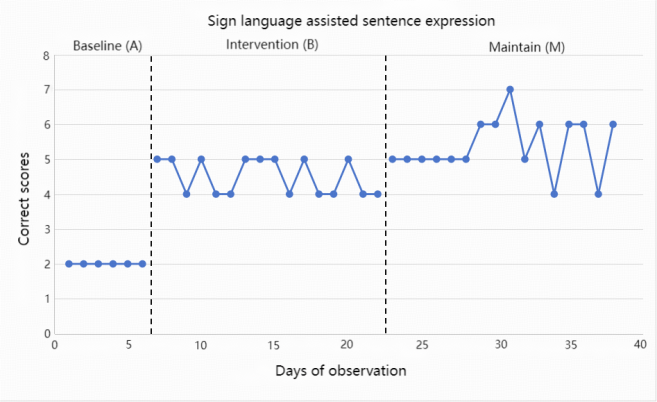
Figure 1: Curve of percentage of correct scores in describing situations in auxiliary aids
Table 1: Effectiveness analysis of augmentative sign language communication
Dimensions of Analysis | Results of analysis | ||
Intra-stage Changes | |||
Stage Name | Baseline period | Intervene period | Maintain Period |
Stage Length | 6 | 16 | 16 |
Level Range | 2-2 | 4-5 | 4-7 |
Level Changes | 0 | 1 | 3 |
Average Level | 2 | 4.5 | 5.4 |
Level Stability | 100% | 100% | 81.25% |
Trend and Data Path within Trends | -(=) | -(=) | /(+) |
Trend Stability | 100% | 100% | 81.25% |
C Value | NA | -0.125 | -0.18 |
Z Value | NA | 0.23 | 0.23 |
Inter-phase Changes | |||
Comparative Stages | Intervention /Baseline period | Maintain /Intervention period | |
Level Changes | 3 | 1 | |
Average Level Changes | 2.5 | 0.9 | |
Trend Changes and Results | —(=)—(=)No change | —(=)/(+)Positive | |
Trend Stability Changes | stable to stable | stable to stable | |
Overlap Rate | 0% | 56.25% | |
C Value | 0.71 | 0.175 | |
Z Value | 3.55** | 0.17 | |
4.2.2. Maintenance effectiveness
As depicted in Figure 1 and Table 1, during the maintenance period the full range of levels is 4-7, with a change of 3 and an average level is 5.4, which shows a stable trend with both level stability and trend stability at 81.25%. According to the results of the C-statistics, the C-value of the maintenance period is -0.18 and the Z-value is 0.23, which does not reach the significant criterion of 0.05, indicating no significant difference and a stable trend without significant change. Transitioning from the intervention period to the maintenance period, the change in level between stages is 1, the change in average level is 0.9, the trend direction changed positively, the trend stability remained stable, and the overlap rate was 100%. According to the results of the in-stage C-statistics, the C-value was 0.175 and the Z-value was 0.17, which did not reach the significant level of 0.05. This indicates no significant difference and suggests that the intervention effects were effectively maintained.
5. Discussion
5.1. Enhancing autistic children's descriptive and social skills in a situation
Before the teaching intervention, participants could only describe a situation using nouns or verbs alone. After the sign language teaching intervention, participant used sign language to assist the use and expression of oral language. First, the participant was able to prompt oral expression through "finger reading", which did not require the use of sign language at this stage, including the use of nouns and some adjectives (mainly related to color). Furthermore, participant also used sign language to assist in prompting or correcting oral expression, including verbs (parts), adjectives (parts), directional prepositions, and quantifiers (if involved). Since the subject's description of certain fragments or characters was not comprehensive, the subject had to rely on self to "make marks" to confirm whether the comprehensive description had been completed. In addition, through a series of teaching interventions, participant was able to improve the ability to express themselves independently in a broad context, no longer limited to the use of nouns or verbs alone, such as actively expressing needs or refusing by using sign language to assist their oral language.
5.2. Enhancing the learning efficiency of autistic children
Due to the presence of a more pronounced language barrier, subject was less effective in purely linguistic learning processes. Prior to the teaching intervention, he/she frequently exhibited problematic behaviours, such as resisting learning by talking out loud about things that are not relevant to learning. Although attempts were made to use positive behavioural support to improve the student's problematic behaviours and negative emotions, learning remained less effective. With the intervention of sign language teaching, the participant was able to understand and use the abstract language in a more visual way by imitating the positional prepositions, verbs, adjectives and quantifiers of the target objects in the context, which in turn improved the learning efficiency.
6. Conclusion
In this study, A-B-M was used as an auxiliary sign language strategy to improve the situation description ability of autistic children. The stability of children's data points using long and short sentences (including nouns, verbs, adjectives, quantifiers, and directional prepositions) in specific situations was observed repeatedly at baseline, followed by an experimental treatment that assisted sign language strategies, and finally, the children's maintenance performance was assessed at the end of the week. However, there are some shortcomings in this paper. First of all, the teaching intervention time of this study should be set for a long time to enhance the familiarity of the subjects. In addition, this study only focuses on the description of parallel relations in the context, and it is suggested that future studies can be further extended to the description of logical relationships such as adversative or transitive relations.
References
[1]. Thunberg, G. (2011). Augmentative and Alternative Communication Intervention for Children with Autism Spectrum Disorders. InTech. doi: 10.5772/18511
[2]. Costescu C, Pitariu D, David C, Rosan A. social Communication Predictors in Autism Spectrum Disorder. Theoretical Review. Journal of Experimental Psychopathology. 2022;13(3). doi:10.1177/20438087221106955
[3]. Taverna, E. C., Huedo-Medina, T. B., Fein, D. A., & Eigsti, I.-M. (2021). The interaction of fine motor, gesture, and structural language skills: The case of autism spectrum disorder. Research in Autism Spectrum Disorders, 86, 101824-. https://doi.org/10.1016/j.rasd.2021.101824
[4]. Thiemann-Bourque, K., Brady, N., McGuff, S., Stump, K., & Naylor, A. (2016). Picture Exchange Communication System and Pals: A Peer-Mediated Augmentative and Alternative Communication Intervention for Minimally Verbal Preschoolers With Autism. Journal of speech, language, and hearing research : JSLHR, 59(5), 1133–1145. https://doi.org/10.1044/2016_JSLHR-L-15-0313
[5]. Frolli, A., Ciotola, S., Esposito, C., Fraschetti, S., Ricci, M. C., Cerciello, F., & Russo, M. G. (2022). AAC and Autism: Manual Signs and Pecs, a Comparison. Behavioral Sciences, 12(10), 359. https://doi.org/10.3390/bs12100359.
[6]. Shield, A., Cooley, F., & Meier, R. P. (2017). Sign Language Echolalia in Deaf Children with Autism Spectrum Disorder. Journal of Speech, Language, and Hearing Research, 60(6), 1622-1634.
[7]. Shan-Chu Cheng (2009) A Comparison of Picture Exchange Communication System and Manual Signs on Teaching Behavioral Language for Children with Severe Autism [Master dissertation, National Hualien University of Education]. National Digital Library of Theses and Dissertations in Taiwan. https://hdl.handle.net/11296/d85gj5
[8]. Goldin-Meadow, S., & Brentari, D. (2017). Gesture, sign, and language: The coming of age of sign language and gesture studies. The Behavioral and Brain Sciences, 40, e46-e46. https://doi.org/10.1017/S0140525X15001247
[9]. Pezzuoli, F., Tafaro, D., Pane, M., Corona, D., & Corradini, M. L. (2020). Development of a New Sign Language Translation System for People with Autism Spectrum Disorder. Advances in Neurodevelopmental Disorders, 4(4), 439–446. https://doi.org/10.1007/s41252-020-00175-6
[10]. Ozyurek, A. (2018). Role of gesture in language processing: Toward a unified account for production and comprehension. In S.-A. Rueschemeyer, & M. G. Gaskell (Eds.), Oxford Handbook of Psycholinguistics (2nd ed., pp. 592-607). Oxford: Oxford University Press. doi:10.1093/oxfordhb/9780198786825.013.25.
[11]. Feng. H, Sun. W. J. , Zhou. W.Q. & Cai. X.H. (2019). Practical Handbook for Teaching Social Emotional and Language Behaviors in Children with Autism. (2nd ed.). Taipei: Psychological Publishing House.
[12]. Niu.W.Y & Wu.Y.Y (2015). Single case study research design and meta-analysis (1st edition). Psychology Press
Cite this article
Deng,L. (2025). An Intervention Study of Augmentative Sign Language on the Ability to Describe Situations in Autistic Children with Speech Impairments. Lecture Notes in Education Psychology and Public Media,86,47-52.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 6th International Conference on Educational Innovation and Psychological Insights
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Thunberg, G. (2011). Augmentative and Alternative Communication Intervention for Children with Autism Spectrum Disorders. InTech. doi: 10.5772/18511
[2]. Costescu C, Pitariu D, David C, Rosan A. social Communication Predictors in Autism Spectrum Disorder. Theoretical Review. Journal of Experimental Psychopathology. 2022;13(3). doi:10.1177/20438087221106955
[3]. Taverna, E. C., Huedo-Medina, T. B., Fein, D. A., & Eigsti, I.-M. (2021). The interaction of fine motor, gesture, and structural language skills: The case of autism spectrum disorder. Research in Autism Spectrum Disorders, 86, 101824-. https://doi.org/10.1016/j.rasd.2021.101824
[4]. Thiemann-Bourque, K., Brady, N., McGuff, S., Stump, K., & Naylor, A. (2016). Picture Exchange Communication System and Pals: A Peer-Mediated Augmentative and Alternative Communication Intervention for Minimally Verbal Preschoolers With Autism. Journal of speech, language, and hearing research : JSLHR, 59(5), 1133–1145. https://doi.org/10.1044/2016_JSLHR-L-15-0313
[5]. Frolli, A., Ciotola, S., Esposito, C., Fraschetti, S., Ricci, M. C., Cerciello, F., & Russo, M. G. (2022). AAC and Autism: Manual Signs and Pecs, a Comparison. Behavioral Sciences, 12(10), 359. https://doi.org/10.3390/bs12100359.
[6]. Shield, A., Cooley, F., & Meier, R. P. (2017). Sign Language Echolalia in Deaf Children with Autism Spectrum Disorder. Journal of Speech, Language, and Hearing Research, 60(6), 1622-1634.
[7]. Shan-Chu Cheng (2009) A Comparison of Picture Exchange Communication System and Manual Signs on Teaching Behavioral Language for Children with Severe Autism [Master dissertation, National Hualien University of Education]. National Digital Library of Theses and Dissertations in Taiwan. https://hdl.handle.net/11296/d85gj5
[8]. Goldin-Meadow, S., & Brentari, D. (2017). Gesture, sign, and language: The coming of age of sign language and gesture studies. The Behavioral and Brain Sciences, 40, e46-e46. https://doi.org/10.1017/S0140525X15001247
[9]. Pezzuoli, F., Tafaro, D., Pane, M., Corona, D., & Corradini, M. L. (2020). Development of a New Sign Language Translation System for People with Autism Spectrum Disorder. Advances in Neurodevelopmental Disorders, 4(4), 439–446. https://doi.org/10.1007/s41252-020-00175-6
[10]. Ozyurek, A. (2018). Role of gesture in language processing: Toward a unified account for production and comprehension. In S.-A. Rueschemeyer, & M. G. Gaskell (Eds.), Oxford Handbook of Psycholinguistics (2nd ed., pp. 592-607). Oxford: Oxford University Press. doi:10.1093/oxfordhb/9780198786825.013.25.
[11]. Feng. H, Sun. W. J. , Zhou. W.Q. & Cai. X.H. (2019). Practical Handbook for Teaching Social Emotional and Language Behaviors in Children with Autism. (2nd ed.). Taipei: Psychological Publishing House.
[12]. Niu.W.Y & Wu.Y.Y (2015). Single case study research design and meta-analysis (1st edition). Psychology Press