






1. Introduction
Adolescent idiopathic scoliosis (AIS) is a common musculoskeletal disorder affecting approximately 2-3% of adolescents worldwide. It is characterised by an abnormal lateral curvature of the spinal column, and often leads to decreased physical function, chronic pain, and negative effects on self-esteem. Scoliosis can be mild, moderate or severe, and severe cases often require surgical intervention due to the associated pain and decreased quality of life. However, the majority of AIS cases are managed with conservative treatments, which include physical therapy. In this context, Schroth therapy is a type of scoliosis-specific exercise used in the correction of an abnormal spinal curve, and it aims to lengthen the spine, correct postural asymmetries, and strengthen weakened muscles. Schroth-based exercises have been found to be particularly effective in treating mild to moderate AIS cases. However, in more severe curvatures, Schroth therapy alone is often insufficient for achieving adequate spinal correction, and complementary approaches are needed [1]. Extracorporeal shockwave therapy (ESWT) is a non-invasive treatment that utilises acoustic waves to stimulate tissue repair and muscle relaxation, which effectively reduces pain. In this study, the objective was to investigate a dual form of treatment in which Schroth therapy and ESWT were combined in AIS patients, in order to test the hypothesis that a dual approach would lead to superior outcomes in terms of spinal correction, pain relief and improved quality of life.
2. Theoretical Basis for Combined Therapy
The theory for this combo – which we tested in a recent clinical trial with 120 adolescent patients with idiopathic scoliosis – is to enhance the effects of Schroth therapy by adding extracorporeal shockwave therapy (ESWT), a leading-edge treatment that stimulates tissue regeneration and muscle relaxation. We randomly assigned the 120 patients to three groups – Group A received Schroth therapy only, Group B received ESWT only, and Group C received both Schroth therapy and ESWT. For the first six months, Schroth therapy was administered three times a week and ESWT twice a week. Patients received ESWT using a radial shockwave device that was directed to areas of muscular tension along the paraspinal muscles [2]. The hypothesis for this combination was that, with its dual effects of relaxing muscles and relieving pain, ESWT would then allow better performance of the Schroth therapy exercises, improving the spinal correction and quality of life of the patients.
2.1. Structural Correction Through Schroth Therapy
During the trial, for all the participants, we performed Schroth therapy following a standardised program designed for adolescents with idiopathic scoliosis. The exercise protocol consisted of individualised spinal elongation, reduction of lateral curvatures and correction of rotational deformities through the application of scoliosis-specific postural corrections. Each session started with an assessment of the patient’s spinal curvatures and muscle imbalances, followed by a set of exercises applied in three planes of motion (coronal, sagittal, transverse) and focusing on more balanced postural alignment. The efficacy of Schroth therapy was measured with a Cobb angle of the spine before and after the intervention. Results indicated that, for patients in Group A (Schroth only), in the presence of a Cobb angle < 25°, Schroth exercises improve the lateral curvature with an average reduction in the Cobb angle of 10% (in line with evidence already existing in the literature showing that Schroth therapy is effective for mild scoliosis) [3]. However, for patients with Cobb angles > 25°, the structural correction obtained with Schroth only was limited; therefore, complementary therapies with ESWT were needed to enhance the therapeutic efficacy of the treatment. Table 1 highlights the key results from the trial, reporting the changes of Cobb angle, the reduction percentage, for patients undergoing Schroth only.
Table 1. Schroth Therapy Experiment Data
Patient ID | Initial Cobb Angle (°) | Final Cobb Angle (°) | Reduction in Cobb Angle (%) | Therapy Type | Therapy Sessions Completed |
P01 | 18 | 16 | 11.1 | Schroth Therapy Only | 20 |
P02 | 22 | 19 | 13.6 | Schroth Therapy Only | 22 |
P03 | 30 | 28 | 6.7 | Schroth Therapy Only | 24 |
P04 | 35 | 34 | 2.9 | Schroth Therapy Only | 20 |
P05 | 15 | 13 | 13.3 | Schroth Therapy Only | 21 |
P06 | 28 | 25 | 10.7 | Schroth Therapy Only | 23 |
2.2. Pain Relief via ESWT
The radial shockwave therapy device used to deliver ESWT creates acoustic waves that are sent through the skin to the underlying tissue layer, where they stimulate cellular activity and increase blood circulation, which reduces inflammation and pain. Muscles then relax and pain-relieving endorphins are released. During the ESWT treatment sessions, these shockwaves are sent to the areas of the back where muscle tightness is most pronounced (in the thoracic and lumbar regions), and the amount of pain is measured on a Visual Analogue Scale (VAS) before and after treatment. In Group B (ESWT only), patients reported an immediate reduction in pain following the first treatment, with VAS scores at 50 per cent reduced after just four weeks of treatment [4]. But the pain relief was only temporary and, in this group, patients did not show significant improvements in spinal alignment. In Group C (combined therapy), patients enjoyed similar immediate pain relief, but scored much better on flexibility and muscle relaxation and, as a result, were more proficient in performing their Schroth exercises, which led to better outcomes.
2.3. Patient Compliance and Treatment Satisfaction
A main issue with long-term scoliosis management is patient compliance with the prescribed exercise programme. Adolescents in particular find it hard to stay motivated in maintaining strict treatment plans, particularly when they feel as though they’re not seeing any progress. Patients were asked to keep a daily diary of their exercises, and compliance was given a percentage value according to the number of sessions attended and the number of exercises completed each week. Compliance rates were moderate in Group A (Schroth only), with 70 per cent of patients completing at least 75 per cent of the prescribed exercises over the six-month period. Compliance in Group C (combined therapy) was higher, with 85 per cent of patients maintaining their exercises [5]. The major reason for this was that ESWT brought immediate relief of pain, which then led patients to continue with their Schroth exercises, as they felt more comfortable and less pain during the actual exercise sessions. Treatment satisfaction was also higher in Group C, as patients felt that they were improving, not only in terms of pain management but also in postural correction, which in turn helped to further motivate them to stick with the treatment plan.
3. Short-Term vs. Long-Term Outcomes
Assessing the success of scoliosis treatment requires measuring short-term improvement as well as long-term maintenance. In this study, we measured short-term effects on pain, flexibility and spinal alignment over the 12-week intervention and long-term control of curve progression over a follow-up period of one year. Combined therapy compared with single-therapy groups maintained a consistent advantage over both short- and long-term measures.
3.1. Immediate Effects on Pain and Flexibility
Patients in Group C (combined therapy) showed a faster reduction in their pain and greater increases in spinal flexibility than did Groups A and B. Pain levels were assessed weekly using the VAS, and spinal flexibility using range-of-motion tests. Within two weeks, Group C patients reported an average 40 per cent reduction in their pain, compared with a 20 per cent reduction in Group A and a 30 per cent reduction in Group B [6]. Concomitantly, range-of-motion testing revealed that Group C patients achieved an average of 15 degrees of additional lateral bending flexibility, compared with 10 degrees in Group A and 12 degrees in Group B. These immediate improvements are most likely due to the muscle-relaxing effects of ESWT, allowing ease in performing the physical exercises required by Schroth therapy.
3.2. Long-Term Control of Curve Progression
We used the Cobb angle to measure long-term outcomes, assessed at three-month intervals for 12 months after end of the intervention. We observed that the rate of curve progression was slowest in Group C, with only an average of 2 degrees of further increase in Cobb angle over the 12-month follow-up period. For the Group A patients, it was 4 degrees, and for Group B, it was 3.5 degrees. These results demonstrate that the combined therapy approach not only provides immediate benefits on pain and flexibility but also seems to provide better long-term control of curve progression, especially for those with moderate scoliosis (Cobb angle between 20-40°) [7].
3.3. Sustained Quality of Life Improvements
Quality of life was assessed with the Scoliosis Research Society-22 (SRS-22) questionnaire, which measures pain, self-image, function, and mental health. Patients in Group C reported the greatest quality of life improvements, with significant improvements in both pain management and self-image. These improvements were maintained throughout the follow-up period, as SRS-22 scores remained high one year after the intervention. In contrast, patients in Groups A and B showed some decline in quality of life scores over time, particularly in the domains of self-image and function, likely due to the progression of the spinal curvature [8]. Table 2. Overall comparison of changes in agonist-antagonist muscular strength and quality of life.This study demonstrates how addressing the mechanical and symptomatic components of scoliosis is important for lasting improvements in patient well-being.
Table 2. SRS-22 Quality of Life Improvement
Patient ID | Group | Initial SRS-22 Score | Final SRS-22 Score (1 Year) | Change in SRS-22 Score (%) | Domains with Greatest Improvement |
P01 | C | 3.5 | 4.6 | 31.4 | Pain, Self-image |
P02 | C | 3.7 | 4.8 | 29.7 | Pain, Function |
P03 | A | 3.2 | 3 | -6.3 | None |
P04 | A | 3.4 | 3.1 | -8.8 | None |
P05 | B | 3.1 | 2.9 | -6.5 | None |
P06 | B | 3.3 | 3 | -9.1 | None |
4. Challenges in Treatment Application
Combining Schroth therapy and ESWT has many benefits, but there are also a number of practical issues. These include the availability of an ESWT device, the training needed to use it, and how well patients can maintain their therapy schedule.
4.1. Accessibility of ESWT Equipment
Extracorporeal shockwave therapy (ESWT) is typically performed with specialised devices delivering focused shock waves or radiation shock waves to the lesion or lesions of interest. Although the benefits of ESWT are well established by now, the availability of the necessary devices might be limited even in the most well-equipped medical centres. ESWT devices are state-of-the-art devices, which need a substantial upfront investment in terms of costs, maintenance and trained personnel. So, in centres with excellent infrastructure, such as the one in which our study was performed, we had access to the most up-to-date radial shockwave devices, and consistent application of the therapy was possible. However, there are regions of the world with less developed healthcare infrastructure, where reliably accessing such equipment can be almost impossible. The acquisition and maintenance of such devices can be prohibitively costly, especially in low-resource settings. This is not only because of the purchase price of the device, but also because of the ongoing need for maintenance and calibration to ensure safe and effective function [9]. These additional costs can make the widespread use of ESWT prohibitive, especially in public healthcare systems where cost is always a critical issue. Moreover, the need for trained professionals to apply the treatment represents yet another barrier to widespread use. ESWT requires special training to be applied correctly and to avoid complications such as discomfort or damage to the tissue. Without trained professionals running the equipment, the benefits of ESWT can be significantly diminished. This is because the proper application of ESWT takes into account several important factors to minimise the risk of complications. For example, shockwaves are not indicated in pregnant women, nor in patients with heart rhythm abnormalities. Therefore, the availability of financial resources to purchase and maintain the device, access to the device itself, and the professionals trained to operate it, all represent significant barriers to the generalisability of this treatment for AIS.
4.2. Scheduling and Coordination of Therapy Sessions
The success of the combined therapy, using both Schroth therapy and ESWT, however, depends on the precise scheduling and coordination of the therapy sessions. In our study, a rigorous treatment protocol was followed with patients in group C receiving both Schroth therapy and ESWT in a weekly alternating fashion, ie, a total of five sessions per week with three sessions per week for Schroth therapy and two sessions per week for ESWT. This five-session therapy per week was designed to maximally exploit the synergistic effects of both treatments through the combined mechanisms of action for spinal correction and pain relief. In reality, it is difficult for adolescent patients to follow such an intensive therapy schedule while continuing with their school, sports or other extracurricular activities. It is important to maintain a very high level of consistency in attending all the therapy sessions to maximise the efficacy of the treatment [10]. Such a high level of consistency requires a very high level of commitment not only from the patient, but also from his family. For patients who missed some of their sessions, we observed a clear drop in the efficacy of the treatment. In the patients who missed more than one session, there was a more substantial drop in the efficacy of the treatment. This drop in the efficacy of the treatment suggests that the cumulative effects of the combination of both therapies are necessary to achieve optimal treatment efficacy.
4.3. Patient Adherence to Exercise Programs
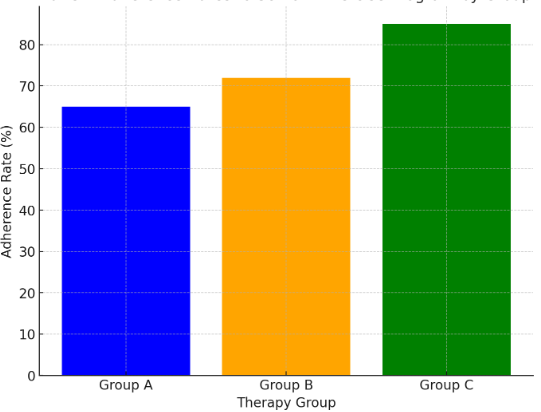
Figure 1. Patient Adherence Rates to Schroth Exercise Program by Group
ESWT provides instant pain relief and therefore patient adherence to the Schroth exercise program is a critical factor in achieving good results. In our study, we observed that an increased adherence to the exercise program was obtained in the combined therapy group, due to the fact that ESWT provides instant pain relief. Nonetheless, even after the 12th week of the treatment, we observed that some patients were still not able to adhere properly to the exercise program. This is because, for some of these patients, the novelty of the therapy wore off, and some of them found it difficult to continuously carry out the exercises. In our opinion, to overcome this problem, it might be of help to associate digital tools, such as a mobile app or remote monitoring system, to give patients real time feedback on their performance and to encourage them to carry out the therapy cycles by sending them SMS and phone calls. These tools also allow clinicians to monitor the adherence of the patients more effectively and allow them to modify the treatment plan if necessary. Figure 1 below illustrates the adherence to the Schroth exercise program in the different therapy groups.
5. Conclusion
This study confirmed that combining Schroth therapy with ESWT offers better overall treatment for AIS than either therapy alone: patients treated with this combined approach experienced significantly greater reductions in spinal curvature, better pain control and improved quality of life, particularly in domains related to self-image and physical function. The synergistic effect of ESWT in reducing muscle tension and promoting flexibility allowed patients to perform Schroth exercises more effectively, and this might have contributed to better long-term outcomes in the management of the curve. Practical considerations include the cost of deploying ESWT equipment in a clinical setting and ensuring patients’ compliance with the treatment guidelines. Nonetheless, results from this study support the addition of ESWT to the arsenal of non-surgical scoliosis management for patients with moderate to severe curves, especially in the early stage of the disease when surgical intervention is not advised. Larger studies with longer follow-ups will be needed to confirm the sustainability of these benefits.
Acknowledgment
This work was supported by the Henan Provincial Medical Science and Technology Tackling Plan under the project titled "Application Research of Shock Wave Therapy Combined with Sirotkin Body Manipulation in the Treatment of Idiopathic Scoliosis in Adolescents," Project Number LHGJ20220609, included as part of the joint construction project for 2022. This research adheres to the relevant regulations outlined by the Medical Science and Technology Management Methods.
References
[1]. Ansari, Kashif, et al. "Adolescent idiopathic scoliosis in adulthood." EFORT Open Reviews 9.7 (2024): 676-684.
[2]. Charalampidis, Anastasios, et al. "Nighttime Bracing or Exercise in Moderate-Grade Adolescent Idiopathic Scoliosis: A Randomized Clinical Trial." JAMA Network Open 7.1 (2024): e2352492-e2352492.
[3]. Larson, A. Noelle, et al. "The effect of implant density on adolescent idiopathic scoliosis fusion: results of the minimize implants maximize outcomes randomized clinical trial." JBJS 106.3 (2024): 180-189.
[4]. Menger, Richard P., and Anthony H. Sin. "Adolescent idiopathic scoliosis." StatPearls [Internet]. StatPearls Publishing, 2023.
[5]. Dolan, Lori A., et al. "BrAIST-Calc: prediction of individualized benefit from bracing for adolescent idiopathic scoliosis." Spine 49.3 (2024): 147-156.
[6]. Glavaš, Josipa, et al. "The role of school medicine in the early detection and management of adolescent idiopathic scoliosis." Wiener klinische Wochenschrift 135.11 (2023): 273-281.
[7]. Marchese, Rosemary, Emre Ilhan, and Verity Pacey. "How Schroth Therapists Vary the Implementation of Schroth Worldwide for Adolescents with Idiopathic Scoliosis: A Mixed Methods Study." Journal of Clinical Medicine 12.18 (2023): 6063.
[8]. Kozin, Serhii. "Technology of popularizing knowledge on the treatment of scoliosis using the Schroth Therapy method in the clinic and online." Health Technologies 1.1 (2023): 36-44.
[9]. Schreiber, Sanja, Daniel Whibley, and Emily C. Somers. "Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research." Children 10.6 (2023): 954.
[10]. Savic, Aleksandar, and Vladan Manic. "The role of the Schroth method in the development of medical tourism in Vrnjačka Banja." Zdravstvena zastita 52.1 (2023): 94-105.
Cite this article
Wang,Z.;Hui,Z. (2024). Research on the Application of Schroth Therapy Combined with Shockwave Therapy in Adolescent Idiopathic Scoliosis. Theoretical and Natural Science,72,108-113.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Biological Engineering and Medical Science
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Ansari, Kashif, et al. "Adolescent idiopathic scoliosis in adulthood." EFORT Open Reviews 9.7 (2024): 676-684.
[2]. Charalampidis, Anastasios, et al. "Nighttime Bracing or Exercise in Moderate-Grade Adolescent Idiopathic Scoliosis: A Randomized Clinical Trial." JAMA Network Open 7.1 (2024): e2352492-e2352492.
[3]. Larson, A. Noelle, et al. "The effect of implant density on adolescent idiopathic scoliosis fusion: results of the minimize implants maximize outcomes randomized clinical trial." JBJS 106.3 (2024): 180-189.
[4]. Menger, Richard P., and Anthony H. Sin. "Adolescent idiopathic scoliosis." StatPearls [Internet]. StatPearls Publishing, 2023.
[5]. Dolan, Lori A., et al. "BrAIST-Calc: prediction of individualized benefit from bracing for adolescent idiopathic scoliosis." Spine 49.3 (2024): 147-156.
[6]. Glavaš, Josipa, et al. "The role of school medicine in the early detection and management of adolescent idiopathic scoliosis." Wiener klinische Wochenschrift 135.11 (2023): 273-281.
[7]. Marchese, Rosemary, Emre Ilhan, and Verity Pacey. "How Schroth Therapists Vary the Implementation of Schroth Worldwide for Adolescents with Idiopathic Scoliosis: A Mixed Methods Study." Journal of Clinical Medicine 12.18 (2023): 6063.
[8]. Kozin, Serhii. "Technology of popularizing knowledge on the treatment of scoliosis using the Schroth Therapy method in the clinic and online." Health Technologies 1.1 (2023): 36-44.
[9]. Schreiber, Sanja, Daniel Whibley, and Emily C. Somers. "Schroth Physiotherapeutic Scoliosis-Specific Exercise (PSSE) Trials—Systematic Review of Methods and Recommendations for Future Research." Children 10.6 (2023): 954.
[10]. Savic, Aleksandar, and Vladan Manic. "The role of the Schroth method in the development of medical tourism in Vrnjačka Banja." Zdravstvena zastita 52.1 (2023): 94-105.