







1. Introduction
Coronary heart disease (CHD) is one of the common cardiovascular diseases [1]. It is a kind of heart disease caused by coronary atherosclerosis, which not only leads to narrowing or blocking of blood vessels and changes in coronary artery function but also leads to myocardial ischemia or necrosis [2]. Globally, approximately 5% of adults over the age of 20 have CHD. In 2021 alone, 19.39 million people died from cardiovascular and cerebrovascular diseases, among which CHD is the most common and important type [3]. Therefore, CHD has been identified as the world's highest mortality disease, which undoubtedly brings a heavy burden to patients' families and society. Its pathogenesis is a highly complex process [4]. In addition to uncontrollable factors such as gender, age, and genes, controllable factors such as blood pressure, smoking, cholesterol, and diabetes also increase the risk of CHD [5]. Of course, with the advancement of medical methods, effective prevention and treatment strategies can be developed by studying the pathogenesis and risk factors of CHD. This not only promotes the development of cardiology but also advances in other fields such as molecular biology and genetics.
There have been many researches conducted relevant studies on the influencing factor of CHD around the world. For instance, the study by Johansen, Vedel-Krogh, Nielsen, Afzal, Davey Smith, & Johansen et al. included 104,867 individuals from the Copenhagen General Population study and conducted a mediation analysis using VanderWeele's method [6]. It was found that elevated residual cholesterol largely explained the increased risk of myocardial infarction and coronary heart disease in individuals with unhealthy lifestyles. Cao & Wu found that healthy lifestyle changes based on exercise could improve multiple risk factors and prevent CHD in the elderly [7]; The use of KNN, decision tree and SVM methods not only confirmed the known influencing factors of CHD, but also found that self-evaluation level of health, income level and education level have potential effects on CHD. Moreover, it is recommended to combine XGBoost and stepwise logistic regression (LR) analysis after data balancing in the CHD risk prediction models [8].
In this article, CHD data, the LR model, and the random forest (RF) model were used to analyze the influencing factors and predict the incidence of CHD. By analyzing the research results, the aim is to put forward relevant suggestions for the prevention of CHD.
2. Method
2.1. Data set
This article uses Kaggle's Heart Disease Dataset, which has been reviewed and verified by the community, and the data annotation is relatively clear, therefore, it has a certain level of reliability [9]. The dataset contains 4238 sets of data. After deleting 595 sets of data with missing values, this study conducts research based on the remaining 3643 sets of data. For the occurrence of coronary heart disease, convert “yes” and “no” to 0 and 1, respectively, to meet the requirements of LR and RF models for binary classification variables.
2.2. Model
LR is a multiple regression method used to analyze the relationship between binary or classification results and multiple influencing factors [10]. A logical function maps the result of linear regression to a probability value to determine the likelihood that the sample belongs to a certain class. LR model based on linear regression model
Where
The RF model is a classifier or regressor that contains multiple decision trees, utilizing the difference and diversity among decision trees to improve the accuracy and stability of decisions. It can effectively reduce the risk of overfitting, have a good tolerance for data anomalies, and evaluate the importance of each feature to the prediction results during the training process.
2.3. Experimental design
2.3.1. LR model
|
Estimate |
Std. Error |
z value |
Pr(>|z|) |
|
|
(Intercept) |
-8.4511 |
0.7074 |
-11.947 |
0.0000*** |
|
Gender/Male |
0.5489 |
0.1101 |
4.984 |
0.0000*** |
|
Age |
0.0614 |
0.0068 |
9.088 |
0.0000 *** |
|
Education post graduate |
0.1350 |
0.1979 |
0.682 |
0.4950 |
|
Education primary school |
0.0109 |
0.1643 |
0.066 |
0.9473 |
|
Education uneducated |
0.2073 |
0.1508 |
1.375 |
0.1691 |
|
Current Smoker |
0.0725 |
0.1567 |
0.463 |
0.6436 |
|
Cigs Per Day |
0.0174 |
0.0062 |
2.794 |
0.0052 ** |
|
Blood pressure medicines (BPMeds) |
0.2051 |
0.2324 |
0.882 |
0.3776 |
|
Prevalent Hypertension (PrevalentHyp) |
0.2425 |
0.1382 |
1.755 |
0.0793 |
|
diabetes |
0.0360 |
0.3156 |
0.114 |
0.9093 |
|
total cholesterol (totChol) |
0.0025 |
0.0011 |
2.183 |
0.0291 * |
|
systolic blood pressure (sysBP) |
0.0152 |
0.0038 |
3.999 |
0.0001*** |
|
Diastolic blood pressure (diaBP) |
-0.0036 |
0.0064 |
-0.551 |
0.5815 |
|
BMI |
0.0039 |
0.0128 |
0.303 |
0.7619 |
|
Heart Rate |
-0.0026 |
0.0042 |
-0.623 |
0.5335 |
|
glucose |
0.0071 |
0.0022 |
3.189 |
0.0014 ** |
Note:***‘p<0.001’;**‘p<0.01’; *‘p<0.05’; . ‘p<0.1’
The summary information output from LR models constructed without standardized data, including model coefficient estimates, standard errors, Z-values, p-values, etc. These statistics can be used to determine whether each independent variable has a significant impact on the dependent variable (CHD attack), in which the estimated value reflects the degree of impact and positive negative relationship, the standard error measure is stable, and the Z-value test coefficient is significantly non-zero. When p<0.05, the independent variable has a significant impact on the probability of CHD attack.
Table 1 shows the results of the LR model, where variables such as gender, age, Education post graduate, Cigs Per Day, prevalentHyp, totChol, sysBP, and glucose have significant effects on the onset of CHD. However, Education primary school, Education uneducated, Current Smoker, BPMeds, diabetes, diaBP, BMI, and Heart Rate have no significant effect on the onset of CHD.
Then, on this basis, the abstract of the LR model constructed with standardized data was output and compared with the unstandardized model to more intuitively compare the relative size of the influence of different independent variables on the incidence of CHD and exclude the impact of variable dimension differences.
2.3.2. RF model
|
%IncMSE |
IncNodePurity |
|
|
age |
19.2325 |
51.1663 |
|
education |
1.2850 |
13.0113 |
|
CurrentSmoker |
5.6541 |
3.8298 |
|
Cigs Per Day |
8.4717 |
21.6815 |
|
BPMeds |
4.3185 |
2.6729 |
|
prevalentHyp |
15.7722 |
7.3107 |
|
diabetes |
3.4415 |
2.2347 |
|
totChol |
7.4441 |
52.5294 |
|
sysBP |
28.6078 |
57.8281 |
|
diaBP |
28.2540 |
50.6748 |
|
BMI |
9.0417 |
56.4464 |
|
Heart Rate |
2.4016 |
39.2694 |
|
glucose |
6.4964 |
51.3779 |
Table 2 shows the importance indicators of the variables in the RF model, including %IncMSE (percentage increase in mean square error) and IncNodePurity (increase in node purity). The greater the value of both, the more important the feature is to the model. Table 2 shows that sys BP, diaBP, and age have a significant impact on the incidence of CHD.
2.3.3. Visualized analysis
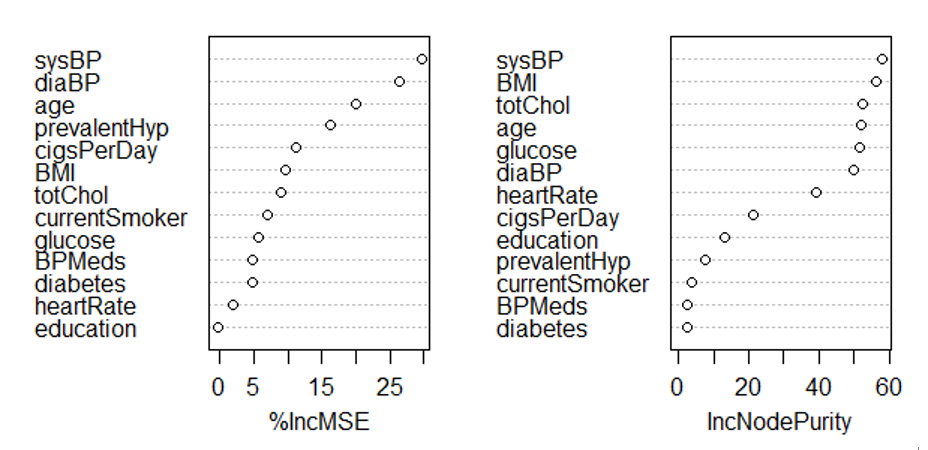
Figure 1 shows the relationship between %IncMSE and IncNodePurity and various variables respectively in the form of scatter plots by using a RF model. Figure 1 measures the importance of variables from the perspectives of model error and node purity and clearly displays the corresponding indicator values for each variable.
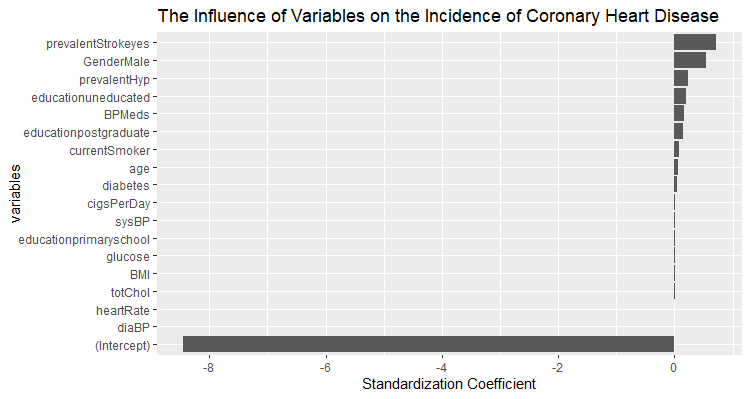
After standardizing the data in Figure 2, the coefficients obtained by fitting the regression model are plotted as the horizontal axis, and each variable is a vertical coordinate, creating a bar chart that eliminates the influence of independent variable dimensions and value ranges. This allows for a direct comparison of the degree of influence of different independent variables on the dependent variable, intuitively reflecting the degree and direction of their influence.
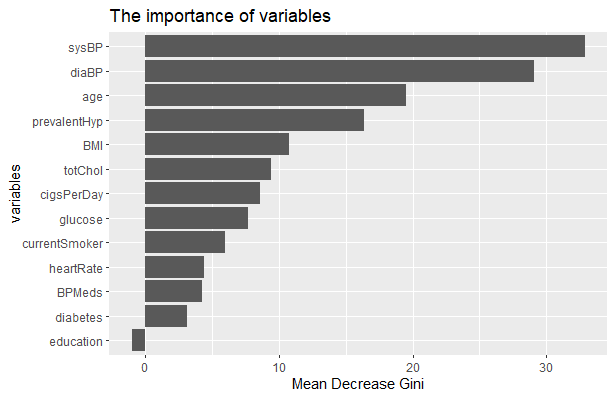
Figure 3 reflects the importance of variables to the incidence of CHD. The ordinate represents the type of variables, and the abscissa represents the average reduction of the Gini index. It is the average value of the Gini index reduction caused by a certain feature as a splitting feature in all decision trees. The larger the value, the stronger the ability of this feature to divide data and reduce impurity, which means the higher the importance of this feature to the model. It can be seen from the above table that the importance of sysBP is relatively important.
2.4. Prediction
First, the experimental data was fitted to the LR model, and then the data set was split according to the proportion of 70% and 30%, among which 70% was the training set and 30% was the prediction set. Then, the constructed model was used for prediction, and prediction probability was obtained. Finally, draw an ROC curve based on the prediction results, as shown in Figure 4.
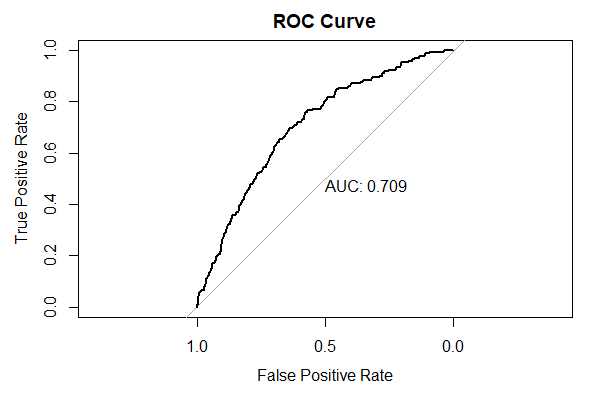
As can be seen from Figure 4, this model has good prediction performance, with the area under the curve (AUC) of 0.709, which is close to 1. Therefore, it can be considered that the model has a strong fitting effect, but it can be further optimized.
3. Conclusion
In this study, it can be seen that CHD is the result of a combination of many factors. In addition to age, gender, and somatic mutations in specific cells (such as DNMT3A, TET2), metabolic abnormalities and unhealthy lifestyles also increase the risk of CHD significantly. Therefore, to reduce the impact of CHD on people's quality of life, controlling blood pressure, glucose, BMI, and total cholesterol, and smoking cessation are the core strategies to prevent its incidence rate. This article demonstrates good performance in predicting CHD based on the LR model. The results show that the area under the ROC curve (AUC) is 0.709, which indicates that the model has a certain ability to distinguish. However, there is still room for optimization in this model, such as introducing more characteristic variables, adjusting data preprocessing methods, or experimenting with nonlinear models to further improve prediction accuracy and generalization.
The Kaggle dataset used in this article has some limitations, which do not indicate the race and source of the experimental samples, so it may affect the ranking of the importance of variables to the incidence of CHD. Some research reports have clearly pointed out that a series of irresistible factors such as race will also have an impact on the incidence of CHD, which may be closely related to their genes and living environment. For example, black people are more likely to suffer from CHD than white people. In the future, further exploration of gene-environment interactions and social factor interventions is also needed to reduce the burden of diseases on individuals, families, and society.
References
[1]. Li, T., Shi, W.T., Wang, G.R., & Jiang, Y.L. 2025. Prevalence and risk factors of frailty in older patients with coronary heart disease: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics, 130, 105721. ISSN 0167-4943.
[2]. Vrints, C., Andreotti, F., Koskinas, K.C., Rossello, X., Adamo, M., Ainslie, J., … ESC Scientific Document Group. 2024. 2024 ESC Guidelines for the management of chronic coronary syndromes. European Heart Journal, 45(36), 3415–3537.
[3]. Ortiz-Ospina, E., & Roser, M. 2016. Global Health. Data adapted from IHME, Global Burden of Disease. https: //ourworldindata.org/grapher/deaths-from-cardiovascular-disease
[4]. Du, J., Wu, W., Zhu, B., Tao, W., Liu, L., Cheng, X., … Pei, K. 2023. Recent advances in regulating lipid metabolism to prevent coronary heart disease. Chemistry and Physical Lipids, 255, 105325.
[5]. National Cholesterol Education Program (US). Expert Panel on Detection and Treatment of High Blood Cholesterol in Adults, 1989. Report of the expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (No. 89). US Department of Health and Human Services, Public Health Service, National Institutes of Health.
[6]. Johansen, M.Ø., Vedel-Krogh, S., Nielsen, S.F., Afzal, S., Davey Smith, G., & Nordestgaard, B.G. 2025. Association of remnant cholesterol with unhealthy lifestyle and risk of coronary heart disease: a population-based cohort study. The Lancet Regional Health – Europe, 10, 101223. ISSN 2666-7762.
[7]. Cao, F., & Wu, X.P. 2024. Lifestyle intervention for the prevention of coronary heart disease in the elderly. Journal of Clinical Cardiology, 40(10), 785–789.
[8]. Yue, H.T., He, C.C., Cheng, Y.Y., Zhang, S.C., Wu, Y., & Ma, J. 2025. Coronary Heart Disease Risk Prediction Model Based on Machine Learning. Chinese General Practice, 28(04), 499–509.
[9]. Kaggle. n.d. Heart disease dataset. https: //www.kaggle.com/datasets/mirzahasnine/heart-disease-dataset
[10]. Wang, Q.Q., Yu, S.C., Qi, X., Hu, Y.H., Zheng, W.J., Shi, J.X., & Yao, H.Y. 2019. Overview of LR model analysis and application. Zhonghua Yu Fang Yi Xue Za Zhi, 53(9), 955–960.
Cite this article
Wang,J. (2025). Influencing Factors and Prediction of Incidence of Coronary Heart Disease. Theoretical and Natural Science,129,91-97.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of ICBioMed 2025 Symposium: Computational Modelling and Simulation for Biology and Medicine
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Li, T., Shi, W.T., Wang, G.R., & Jiang, Y.L. 2025. Prevalence and risk factors of frailty in older patients with coronary heart disease: A systematic review and meta-analysis. Archives of Gerontology and Geriatrics, 130, 105721. ISSN 0167-4943.
[2]. Vrints, C., Andreotti, F., Koskinas, K.C., Rossello, X., Adamo, M., Ainslie, J., … ESC Scientific Document Group. 2024. 2024 ESC Guidelines for the management of chronic coronary syndromes. European Heart Journal, 45(36), 3415–3537.
[3]. Ortiz-Ospina, E., & Roser, M. 2016. Global Health. Data adapted from IHME, Global Burden of Disease. https: //ourworldindata.org/grapher/deaths-from-cardiovascular-disease
[4]. Du, J., Wu, W., Zhu, B., Tao, W., Liu, L., Cheng, X., … Pei, K. 2023. Recent advances in regulating lipid metabolism to prevent coronary heart disease. Chemistry and Physical Lipids, 255, 105325.
[5]. National Cholesterol Education Program (US). Expert Panel on Detection and Treatment of High Blood Cholesterol in Adults, 1989. Report of the expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (No. 89). US Department of Health and Human Services, Public Health Service, National Institutes of Health.
[6]. Johansen, M.Ø., Vedel-Krogh, S., Nielsen, S.F., Afzal, S., Davey Smith, G., & Nordestgaard, B.G. 2025. Association of remnant cholesterol with unhealthy lifestyle and risk of coronary heart disease: a population-based cohort study. The Lancet Regional Health – Europe, 10, 101223. ISSN 2666-7762.
[7]. Cao, F., & Wu, X.P. 2024. Lifestyle intervention for the prevention of coronary heart disease in the elderly. Journal of Clinical Cardiology, 40(10), 785–789.
[8]. Yue, H.T., He, C.C., Cheng, Y.Y., Zhang, S.C., Wu, Y., & Ma, J. 2025. Coronary Heart Disease Risk Prediction Model Based on Machine Learning. Chinese General Practice, 28(04), 499–509.
[9]. Kaggle. n.d. Heart disease dataset. https: //www.kaggle.com/datasets/mirzahasnine/heart-disease-dataset
[10]. Wang, Q.Q., Yu, S.C., Qi, X., Hu, Y.H., Zheng, W.J., Shi, J.X., & Yao, H.Y. 2019. Overview of LR model analysis and application. Zhonghua Yu Fang Yi Xue Za Zhi, 53(9), 955–960.