







1. Introduction
As one of the main sources of energy, sugar ensures the metabolism of the body and maintains the maintenance of the body's blood sugar. Prolonged high or low blood sugar can have an impact on the normal functioning of the body's organs. Insufficient sugar intake can produce symptoms such as dizziness and depression, while high blood sugar can lead to metabolic diseases such as obesity and diabetes mellitus. Over the past few decades, diabetes has been recognized as the most common endocrine disease in the world, and one of the major reasons is that the body becomes resistant to insulin. It is hoped that artificial sweeteners can be used instead of sugar to achieve a reduction in sugar intake without compromising the need for sweetness. To date, the FDA has approved seven non-nutritive sweeteners, including aspartame, stevia, and sodium saccharin, to control the spread of metabolic diseases. However, the available research suggests two opposing views. Some scholars believe that artificial sweeteners can help the body balance metabolic energy, while other researchers see it as a great challenge to overcome inertia.
This paper aims to investigate the existing literature on the relationship between artificial sweetener intake and consumption and obesity, insulin resistance, gestational diabetes and geriatric diabetes. The main studies studied in the evaluation are relevant trials and observational studies, and the comparison of different literature to obtain a more reliable result achievable at the present-day experimental level.
2. Artificial sweeteners and obesity
Over the past few decades, overweight and obesity rates in not just adults, but also children and adolescents have shown a clear upward trend globally [1]. This is worrying because they increase the risk of chronic diseases and can be debilitating, including cardiovascular disease and diabetes [2]. There are many factors that can lead to an increasing number of obesities, including poor eating style and a small amount of physical activity. In the early days, when it was found that artificial sweeteners can provide sweetness without energy intake, they have also been widely used in medical treatment, but with long-term experiments of people, they have found that the use of artificial sweeteners in large quantities may cause metabolic diseases, the most significant of which is obesity. In the last few years, with the increasing use of artificial sweeteners, the phenomenon of weight gain has become more and more obvious, and people have paid more and more attention to related research.
Over the years, some animal experiments have confirmed that artificial sweeteners may have an impact on energy balance. When animals receive signals from artificial sweeteners, they lose the ability to regulate energy and gain weight because artificial sweeteners do not contain energy. Many experiments prove that artificial sweeteners effect appetite. One experiment initiated with a small experiment, it compared drinking water with drinking artificial sweeteners, and the results proved that artificial sweeteners are more likely to cause hunger than water, but did not confirm that they increase food intake. While these are all results from animal models, humans are equally applicable. Studies have shown that people who consume artificial sweeteners for a long time have an increase in BMI index, abdominal fat deposits and high obesity compared with those who do not consume artificial sweeteners.
Adolescents are less likely than adults to control their intake of sugar-flavored foods and beverages. From the early stages of life, sweets trigger behavioral responses that indicate that they are very pleasurable, and many newborns in mammals show a strong preference for sweetness relative to water. While a strong preference may not equal more sweetening, current research shows that children and adolescents do have more intake in sweetened drinks or diets. For example, about 70% of children aged 2-19 currently drink sugary drinks daily [3, 4]. The link between sugary drink intake and obesity has raised awareness of reduced consumption in children. Although artificial sweeteners are given the hope of achieving healthier purposes, they do not achieve the desired results. One intervention study for overweight adolescents showed that those who regularly consumed sugary drinks did lead to a decrease in weight gain compared to the control group. However, this experiment emphasizes the intake of sugar-free drinks rather than beverages with artificial sweeteners, which means that there is no basis for the conclusion that artificial sweeteners will work in humans. Another clinical trial looked at the effect of replacing sugary drinks with drinks containing artificial sweeteners, mainly skinny Dutch children aged 4-11 years, who needed at least one sugary drink to be consumed daily [5]. The results showed that children in the ASB group had less weight gain than those who consumed sugary drinks. But this did not include groups that did not drink sweet drinks every day.
Among adults, existing studies are also controversial, with some arguing that artificial sweeteners are effective in controlling obesity, while in interventional studies, the results do not fully indicate that promoting weight loss in overweight individuals will be due to the specific role of artificial sweeteners themselves. A study of overweight adults surveyed consumers who took sugary drinks every day and were encouraged to replace sugary drinks with sugar-free soda or water; In the absence of specific recommendations for beverage intake, weight loss in both groups was no different from that observed in the control group [6]. Therefore, the best way to improve obesity should be to strictly control the addition of sweeteners by enterprises, whether sucrose or artificial sweeteners.
3. Artificial sweeteners and insulin resistance
From the perspective of the effect of artificial sweeteners on the metabolism of the body, the existing studies have revealed two main aspects: their effects on intestinal composition and energy balance. In a cross-sectional study, the researchers divided diabetics into two groups, Group A who regularly consumed artificial sweeteners and Group B who did not consume them, and both groups were tested for blood glucose levels and serum insulin tests in a fasting state, and then the insulin resistance of each group was calculated with HOMA-IR. The results of the study showed that the values of Group A ranged from 0.9-24.33, the values of Group B ranged from HOMA-IR 0.12-10.83, and the averages of the two groups were 7.39 and 2.9, respectively. The results amply show that people who consume artificial sweeteners have higher insulin resistance [7].
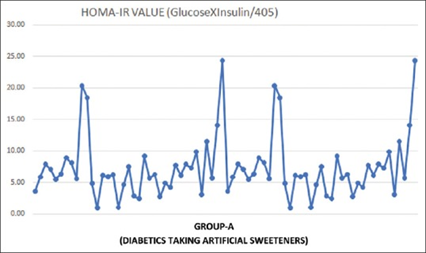
Figure 1. HOMA-IR value from diabetics taking AS.
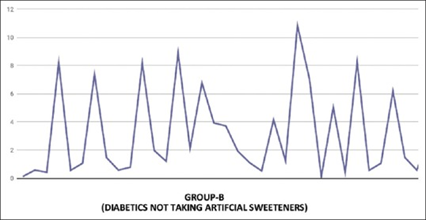
Figure 2. HOMA-IR value from diabetics not taking AS.
A 2014 article published in Nature similarly made a demonstration of glucose intolerance to artificial sweeteners. Suez et al. found that regular consumption of the sweeteners saccharin, sucralose, or aspartame increased poor glucose tolerance in mice by increasing the use of artificial sweeteners as a dietary change. They tested whether artificial sweetener consumption leads to glucose intolerance by subjecting mice to 11 weeks of artificial sweetener intake, followed by transferring the intestinal microbiota of artificial sweetener-fed control mice to germ-free mice with a completely sterile gastrointestinal tract. The study of transferring microorganisms into sterile mice provides a good opportunity to test the effect of the commensal flora on host physiology. This approach has been highly successful in determining how gut microbiota affects host metabolism under disturbed conditions. Suez and his colleagues found that germ-free mice inoculated with NAS-fed microbiota were more intolerant to glucose than mice inoculated with control microbiota. This demonstrates that the gut microbiota can be affected in some way [8].
Similar to Suez et al., other rodent studies have shown that in rodent studies and in vitro experiments, saccharin, potassium acesulfonate, and sucralose may increase the inflammatory response. In addition, by limiting the proliferation and expansion of adipose tissue, inflammatory molecules can inhibit fat production. Thus, lipid spillover and fat accumulation in non-adipose tissue are formed by a decrease in fat cell renewal and adipose tissue expansion. Cellular function may be disrupted by the accumulation of ectopic fats and biologically active lipid metabolites, eventually leading to a decline in functions such as insulin resistance.
4. Artificial sweeteners and intestinal metabolism
Many aspects of human health are related to the intestinal flora and the resulting microbial fermentation products [9]. In addition to fermented and indigestible food components, more such as energy balance and metabolism are closely related to the gut microbiome [10]. Diet is an important regulatory factor that affects a person's overall health. The composition of the intestinal flora may be altered by artificial sweeteners, which was increased in a cross-sectional study of morbidly obese people [11]. In addition, another related cross-sectional study showed that the intake of aspartame or acesulfame potassium did not have an effect on bacterial abundance spectrum or predicted gene function. However, in reality, there is a different bacterial diversity between those who ingest aspartame or acesulfame potassium than people who do not consume these two artificial sweeteners [12].
Among artificial sweeteners, saccharin is a typical example of a category that is commonly used and has been shown in existing studies to affect intestinal metabolism. Saccharin can be divided into three forms: in combination with sodium or calcium, or in acid form. Sodium salt is the most common form of saccharin because of its high solubility and stability. Similar to the effect of acesulfame potassium, the body is unable to metabolize saccharin. After ingestion, about 85-95% of saccharin is absorbed by the body and combined with plasma proteins and distributed in the blood [13] and excreted in the urine. In contrast, 5-15% pass completely through the gastrointestinal tract and are excreted in the feces in their original form. Therefore, the composition of the gut microbiota is affected by a small part of saccharin that is not rapidly absorbed. In addition, sucralose is a class of artificial sweeteners that affects intestinal metabolism. It is structurally very similar to sucrose, but much sweeter than sucrose, about 600 times sweeter. Because sucrose does not digest in the body, even if it is made of sugar, it does not provide calories [14]. The majority of sucralose is eliminated directly in the feces through the gastrointestinal tract. However, it has been found that sucralose can affect the microbiota through its bacteriostatic effect [15].
5. Artificial sweeteners and gestational diabetes mellitus
To ensure an adequate supply of nutrients to the growing fetus, insulin resistance is gradually developed during pregnancy [16]. In women with gestational diabetes mellitus (GDM), hyperglycemia can arise due to insulin resistance. The fetus is able to receive glucose through the placenta, which stimulates the secretion of insulin from the fetus, allowing the fetus to grow more rapidly, resulting in large for gestational age infant (LGA) children [17]. In the short term, the risk of a bad pregnancy increases due to GDM, which is a long-term risk for both mother and offspring with obesity and type II diabetes [18]. The prevalence of GDM is on the rise, as is the need to inhibit its onset and prevention. Artificial sweeteners are one of the ways people are trying to find alternatives to sucrose intake that can inhibit gestational diabetes. In one clinical trial, 376 pregnant women were evaluated continuously for up to a year. Their intake of NNS is mainly derived from non-nutritionally sweetened soft drinks (NNSSDs). According to the study, the number of GDM was found to be higher among NNSSD users than among NNSSD non-users (Figure 3), and diagnostic fasting glucose (FPG) levels were also more common among NNSSD users diagnosed with GDM. [19].
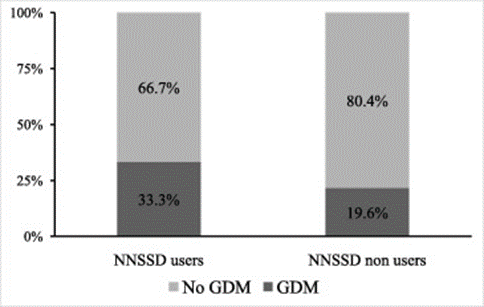
Figure 3. The number of GDMs in NNSSD users and non-users.
In addition, several studies have confirmed that regular consumption of artificial sweeteners during pregnancy increases the risk of preterm delivery compared to pregnant women who do not consume artificial sweeteners. First, most artificial sweeteners are not directly digested, which may alter the composition of the intestinal microbiota. Animal studies show that prenatal consumption of artificial sweeteners leads to changes in the composition of the gut microbiome. When the maternal inflammatory state changes from physiological to excessive levels due to excessive consumption of artificial sweeteners, vascular dysfunction of the placental tissue develops, leading to adverse reactions such as preterm birth. These data suggest that a small increase in birth weight is associated with an increased risk of having an LGA baby. Studies in rodents have found that some artificial sweeteners can activate type 1 sweet taste receptors in the intestine, which may upregulate glucose transporter protein expression and increase intestinal absorption of glucose, thereby promoting insulin secretion. And due to the daily intake of artificial sweeteners will lead to increased maternal glucose levels, which may lead to accelerated fetal growth. Finally, unlike nutritional sweeteners, consumption of non-nutritious artificial sweeteners does not alter the release of satiety-related hormones such as auxin-releasing peptides, peptides YY, and glucose-dependent insulin-stimulating peptides. This may increase the demand for food and lead to an increase in infant birth weight. The effect of artificial sweeteners on birth weight and fetal overgrowth deserves further study as few people have studied LGA-related aspects of the field. For the current study, there are potential factors in antenatal use of artificial sweeteners to increase the risk of allergies in children; However, limited reported data is not sufficient to fully support this view.
Overall, the emergence and development of GDM may be affected by the use of NNSSD and pose a risk of GDM independent of tradition. Even if this study does not directly explore the relationship between NNS and gestational diabetes, commonly used NNS preparations can alter the regulatory metabolism of the intestine and activate the sweet taste receptors in the intestine, thereby affecting glucagon-like peptide 1 (GLP-1), and mechanisms such as this can also reflect the increased risk of GDM in NNS.
6. Artificial sweeteners and older people
Similarly, older people are at high risk for diabetes. In the United States, about $300 billion is spent annually on the treatment of people with diabetes, most of which goes to older adults with long-term diabetes and serious complications. NutriNet-Santé cohort found that beverages containing artificial sweeteners were associated with an increased risk of cardiovascular disease. The WHO 2022 report on the health effects of artificial sweeteners has observed that some adverse effects can be caused by the consumption of beverages containing artificial sweeteners, especially for older diabetics, including a moderate increase in total cholesterol to HDL cholesterol ratio and the risk of hypertension. International health authorities have also found an association between CVD mortality, cardiovascular events and stroke rates and the increasing demand for beverages containing artificial sweeteners. However, the available studies are insufficient to fully argue this point, and the World Health Organization believes that the evidence for these associations remains small.
Elderly people with diabetes are more likely to develop complications such as cardiovascular disease. Postprandial hyperglycemia is a prominent feature of type 2 diabetes in older adults [20]. However, Ferland et al. did a study of patients with type 2 diabetes and found that breakfasts containing aspartame led to higher glucose and insulin levels after consumption. A subsequent study of sucralose, an artificial sweetener, also found that glucose increased significantly after sucralose intake compared to water intake, and insulin secretion increased by about 20%. This is very detrimental for older people with diabetes. Therefore, the elderly, especially those with diabetes, should pay more attention to the intake of artificial sweeteners.
7. Conclusion
Based on this, people should continue to look for more optimized experimental protocols to explore the harm and potential side effects of artificial sweeteners to the human body. Assuming that more research results can overturn the previous remarks about the harm of artificial sweeteners on metabolism, then consumers, especially diabetics and obese people, can eat foods containing artificial sweeteners with more confidence, after all, according to research, artificial sweeteners have exceeded people's imagination to cover a wide range of foods, and even in surface drinking water has been detected quite a lot. Assuming that the research results can further confirm the harm of artificial sweeteners, the state should strictly control the use of artificial sweeteners to prevent them from having deeper harm to the human body and prompt researchers to find sweetener additives that are more conducive to the prevention of diabetes or more friendly to diabetic patients, which is also extremely beneficial to prevent the growth of diabetes. At the same time, for modern enterprises, it is necessary to be more cautious about the addition and use of artificial sweeteners to ensure that consumers will not be affected by artificial sweeteners under the existing technology. In addition, it is more important to improve people's vigilance about the intake of artificial sweeteners, so that people can prevent diabetes and obesity and other related diseases if they do not have artificial sweeteners, artificial sweeteners are not the best choice for diabetic patients to feel sweet, for high-risk groups and ultra-obese patients who have already suffered from diabetes, they should be more cautious about using related products.
References
[1]. K. M. Flegal, M. D. Carroll, B. K. Kit, et al., "Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010," Jama, 307(5), 491-497 (2012).
[2]. M. Ng, T. Fleming, M. Robinson, et al., "Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013," The lancet, 384(9945), 766-781 (2014).
[3]. E. Han,L. M. Powell, "Consumption patterns of sugar-sweetened beverages in the United States," Journal of the Academy of Nutrition and Dietetics, 113(1), 43-53 (2013).
[4]. M. S. Mesirow,J. A. Welsh, "Changing beverage consumption patterns have resulted in fewer liquid calories in the diets of US children: National Health and Nutrition Examination Survey 2001-2010," Journal of the Academy of Nutrition and Dietetics, 115(4), 559-566. e4 (2015).
[5]. J. C. de Ruyter, M. R. Olthof, J. C. Seidell, et al., "A trial of sugar-free or sugar-sweetened beverages and body weight in children," New England Journal of Medicine, 367(15), 1397-1406 (2012).
[6]. D. F. Tate, G. Turner-McGrievy, E. Lyons, et al., "Replacing caloric beverages with water or diet beverages for weight loss in adults: main results of the C hoose H ealthy O pt i ons C onsciously E veryday (CHOICE) randomized clinical trial," The American journal of clinical nutrition, 95(3), 555-563 (2012).
[7]. K. Mathur, R. K. Agrawal, S. Nagpure, et al., "Effect of artificial sweeteners on insulin resistance among type-2 diabetes mellitus patients," Journal of family medicine and primary care, 9(1), 69-71 (2020).
[8]. J. Suez, T. Korem, D. Zeevi, et al., "Artificial sweeteners induce glucose intolerance by altering the gut microbiota," Nature, 514(7521), 181-186 (2014).
[9]. E. E. Canfora, R. C. Meex, K. Venema, et al., "Gut microbial metabolites in obesity, NAFLD and T2DM," Nature Reviews Endocrinology, 15(5), 261-273 (2019).
[10]. S. M. Jandhyala, R. Talukdar, C. Subramanyam, et al., "Role of the normal gut microbiota," World journal of gastroenterology: WJG, 21(29), 8787 (2015).
[11]. P. G. Farup, S. Lydersen,J. Valeur, "Are nonnutritive sweeteners obesogenic? Associations between diet, faecal microbiota, and short-chain fatty acids in morbidly obese subjects," Journal of Obesity, 2019 (2019).
[12]. C. L. Frankenfeld, M. Sikaroodi, E. Lamb, et al., "High-intensity sweetener consumption and gut microbiome content and predicted gene function in a cross-sectional study of adults in the United States," Annals of epidemiology, 25(10), 736-742. e4 (2015).
[13]. B. A. Magnuson, M. C. Carakostas, N. H. Moore, et al., "Biological fate of low-calorie sweeteners," Nutrition Reviews, 74(11), 670-689 (2016).
[14]. S. Chattopadhyay, U. Raychaudhuri,R. Chakraborty, "Artificial sweeteners–a review," Journal of food science and technology, 51(4), 611-621 (2014).
[15]. Omran, G. Ahearn, D. Bowers, et al., "Metabolic effects of sucralose on environmental bacteria," Journal of toxicology, 2013 (2013).
[16]. D. Sonagra, S. M. Biradar, K. Dattatreya, et al., "Normal pregnancy-a state of insulin resistance," Journal of clinical and diagnostic research: JCDR, 8(11), CC01 (2014).
[17]. P. G. Ovesen, J. Fuglsang, M. B. Andersen, et al., "Temporal trends in gestational diabetes prevalence, treatment, and outcomes at Aarhus University Hospital, Skejby, between 2004 and 2016," Journal of diabetes research, 2018 (2018).
[18]. L. L. Kurtzhals, S. K. Nørgaard, A. L. Secher, et al., "The impact of restricted gestational weight gain by dietary intervention on fetal growth in women with gestational diabetes mellitus," Diabetologia, 61(12), 2528-2538 (2018).
[19]. F. Nicolì, A. Prete, F. Citro, et al., "Use of non-nutritive-sweetened soft drink and risk of gestational diabetes," Diabetes Research and Clinical Practice, 178, 108943 (2021).
[20]. E. Szoke, M. Z. Shrayyef, S. Messing, et al., "Effect of aging on glucose homeostasis: accelerated deterioration of β-cell function in individuals with impaired glucose tolerance," Diabetes care, 31(3), 539-543 (2008).
Cite this article
Han,Y. (2023). Analysis of The Effects of Artificial Sweeteners on Diabetes and Obesity. Theoretical and Natural Science,4,32-38.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Biological Engineering and Medical Science (ICBioMed 2022), Part II
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. K. M. Flegal, M. D. Carroll, B. K. Kit, et al., "Prevalence of obesity and trends in the distribution of body mass index among US adults, 1999-2010," Jama, 307(5), 491-497 (2012).
[2]. M. Ng, T. Fleming, M. Robinson, et al., "Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013," The lancet, 384(9945), 766-781 (2014).
[3]. E. Han,L. M. Powell, "Consumption patterns of sugar-sweetened beverages in the United States," Journal of the Academy of Nutrition and Dietetics, 113(1), 43-53 (2013).
[4]. M. S. Mesirow,J. A. Welsh, "Changing beverage consumption patterns have resulted in fewer liquid calories in the diets of US children: National Health and Nutrition Examination Survey 2001-2010," Journal of the Academy of Nutrition and Dietetics, 115(4), 559-566. e4 (2015).
[5]. J. C. de Ruyter, M. R. Olthof, J. C. Seidell, et al., "A trial of sugar-free or sugar-sweetened beverages and body weight in children," New England Journal of Medicine, 367(15), 1397-1406 (2012).
[6]. D. F. Tate, G. Turner-McGrievy, E. Lyons, et al., "Replacing caloric beverages with water or diet beverages for weight loss in adults: main results of the C hoose H ealthy O pt i ons C onsciously E veryday (CHOICE) randomized clinical trial," The American journal of clinical nutrition, 95(3), 555-563 (2012).
[7]. K. Mathur, R. K. Agrawal, S. Nagpure, et al., "Effect of artificial sweeteners on insulin resistance among type-2 diabetes mellitus patients," Journal of family medicine and primary care, 9(1), 69-71 (2020).
[8]. J. Suez, T. Korem, D. Zeevi, et al., "Artificial sweeteners induce glucose intolerance by altering the gut microbiota," Nature, 514(7521), 181-186 (2014).
[9]. E. E. Canfora, R. C. Meex, K. Venema, et al., "Gut microbial metabolites in obesity, NAFLD and T2DM," Nature Reviews Endocrinology, 15(5), 261-273 (2019).
[10]. S. M. Jandhyala, R. Talukdar, C. Subramanyam, et al., "Role of the normal gut microbiota," World journal of gastroenterology: WJG, 21(29), 8787 (2015).
[11]. P. G. Farup, S. Lydersen,J. Valeur, "Are nonnutritive sweeteners obesogenic? Associations between diet, faecal microbiota, and short-chain fatty acids in morbidly obese subjects," Journal of Obesity, 2019 (2019).
[12]. C. L. Frankenfeld, M. Sikaroodi, E. Lamb, et al., "High-intensity sweetener consumption and gut microbiome content and predicted gene function in a cross-sectional study of adults in the United States," Annals of epidemiology, 25(10), 736-742. e4 (2015).
[13]. B. A. Magnuson, M. C. Carakostas, N. H. Moore, et al., "Biological fate of low-calorie sweeteners," Nutrition Reviews, 74(11), 670-689 (2016).
[14]. S. Chattopadhyay, U. Raychaudhuri,R. Chakraborty, "Artificial sweeteners–a review," Journal of food science and technology, 51(4), 611-621 (2014).
[15]. Omran, G. Ahearn, D. Bowers, et al., "Metabolic effects of sucralose on environmental bacteria," Journal of toxicology, 2013 (2013).
[16]. D. Sonagra, S. M. Biradar, K. Dattatreya, et al., "Normal pregnancy-a state of insulin resistance," Journal of clinical and diagnostic research: JCDR, 8(11), CC01 (2014).
[17]. P. G. Ovesen, J. Fuglsang, M. B. Andersen, et al., "Temporal trends in gestational diabetes prevalence, treatment, and outcomes at Aarhus University Hospital, Skejby, between 2004 and 2016," Journal of diabetes research, 2018 (2018).
[18]. L. L. Kurtzhals, S. K. Nørgaard, A. L. Secher, et al., "The impact of restricted gestational weight gain by dietary intervention on fetal growth in women with gestational diabetes mellitus," Diabetologia, 61(12), 2528-2538 (2018).
[19]. F. Nicolì, A. Prete, F. Citro, et al., "Use of non-nutritive-sweetened soft drink and risk of gestational diabetes," Diabetes Research and Clinical Practice, 178, 108943 (2021).
[20]. E. Szoke, M. Z. Shrayyef, S. Messing, et al., "Effect of aging on glucose homeostasis: accelerated deterioration of β-cell function in individuals with impaired glucose tolerance," Diabetes care, 31(3), 539-543 (2008).