






1. Introduction
In today’s anxia-ridden society, panic disorder, an accessory disorder, also affects many groups. After a period of study and comparison, it was found that the research on drug treatment of this disease was not highly concerned at the social level, and there were few treatment cases and targeted studies. Therefore, the topic of this paper is to explore the effects of SSRIs and two of the most common benzodiazepines, fluoxetine and alprazolam, on panic disorder. It is intended to expand the cognitive scope of the treatment of this disease, and provide effective drug comparative studies for patients with panic disorder, so as to facilitate the reference of drug selection. In addition to in-depth research and analysis of the effects of these two drugs, this study aims to help the progress of drug research for panic disorder and aims to win more social attention for patients with panic disorder, providing support and help for patients from both drug treatment and social attention.
2. Review of Panic Disorder
About 2-3% of people suffer from panic attacks. Seven percent of patients had suicidal thoughts or behaviors [1]. This disease is briefly described in the following paragraphs.
2.1. Symptoms of panic disorder.
The symptoms of panic disorder are varied and are described in detail in the DSM-5. Common symptoms can be heart palpitations, suffocation, body tremors, depersonalization, or fear of death [2].
According to the textbook “Psychiatry” published by China People’s Medical Publishing House, symptoms above can be summarized into three of the most common clinical symptoms: panic attacks, apprehensive expectation and avoidance behavior
2.1.1. Panic attack. Panic attack refers to when a patient feels sudden fear and tension, accompanied by a strong sense of loss of control and near-death and occurs in the absence of a special terror environment. At the same time, most patients have symptoms of autonomic disorders, including chest tightness, shortness of breath, and tremors. These symptoms usually last about 20-30 minutes, and have not been recorded for more than an hour.
2.1.2. Apprehensive expectation. Apprehensive expectation refers to when patient in the interval after the onset of the disease is still worried about the recurrence of the disease. However, in this condition, the patient’s experience of anxiety is not prominent, but is replaced by weakness, and the symptoms can take hours to days to fully recover.
2.1.3. Avoidance behavior. Avoidance behavior occurs when the patient suffers from constant anxiety and concern over a recurrence of the illness, and consequently avoids places such as school and their workplace. for fear of the unfortunate consequences of the illness. Avoidance behavior does not occur in all patients, only about 60% [1].
2.2. Impact of Panic Disorder
Studies in Europe and the United States have shown that 2-3% of adults develop panic disorder within a 12-month period, and this rate is significantly lower in Latinos, African-Americans and Asian-Americans than in whites and Native Americans. Experimental data in countries in Asia, Africa and Latin America show that the number of cases during the same period is as low as 0.1-0.8%. In all regions, the incidence is mainly during adolescence or post-adolescence adulthood, and the incidence is not high in children or the elderly (less than 0.4% before 14 years of age and less than 0.7% after 67 years of age) [2]. Most of the time panic disorder is not a lifelong disease, only more than 6 months of the course of the disease can become chronic. 30% of patients diagnosed with panic disorder have a good response within a few years and no recurrence, 25% have an intermittent course, 45% have a relatively poor response, and about 7% have suicidal tendencies or behaviors [1].
2.3. History of Panic disorder
Panic disorders were not recognized by the American Psychiatric Association nor included in the DSM-111 until 1980. Before that, patients were often diagnosed as “stressed” or “nervous.” Due to a lack of understanding among health professionals about all anxiety disorders, including panic disorder, few receive effective treatment. Although anxiety disorders have only recently been officially recognized, they have been around throughout human history. The word fear first comes from the name of Pan in ancient Greek mythology. It is said that he can make people who occupy his territory feel a sudden great fear, so people call this feeling “panic” [3]. In the second half of the 19th century, the field of anxiety symptoms began to change gradually. When the word “panic” was first used in psychiatry in 1879, Henry Maudsley, in his book The Physiology and Pathology of the Mind, describes much of the knowledge of insanity and a depressive panic [4]. In 1964, Donald Klein published an article stating that patients with panic attacks do not realize the difference between the disorder and generalized anxiety disorder because chronic anxiety masks the specificity of panic attacks [5]. His observations and descriptions influenced the third edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III, 1980), in which the term panic disorder first appeared in an official classification. Over the past 50 years, people have uncovered the mysteries of panic disorder through basic and clinical research [6].
2.4. Causes of Panic disorder
Panic attacks are easy to cause, and most people have experienced panic or fear at some point in their lives. These brief episodes can be triggered by a variety of factors, such as sudden shock. But when panic attacks turn into panic disorder, the cause of the illness changes. While researchers are still uncertain about the causes, common theories include genetics, CO2 hypersensitivity, and psychosocial factors.
I. genetic
In studying the genetic causes of panic disorder, researchers have chosen two methods: family studies and twin studies. Family studies examined clusters of depressive disorders by comparing phenotypic prevalence between preexisting relatives and control relatives without the disease. The researchers found that when the first degree relative of the first panic disorder was younger than 20 years old, the family risk increased by 17 times. Over the age of 20, the risk increases six-fold. Although this study demonstrates the clustering of the disease in families, the process of genetic and environmental factors is not well distinguished, resulting in significant limitations. Twin studies complement family studies, and twin studies of panic disorder show that the disorder is moderately heritable, and that identical twins are more likely to have it than fraternal twins. Researchers estimate the heritability of the disease to be 30 to 40%. A recent study of 5,000 twins in Virginia showed a heritability of about 0.28 for panic disorder [7].
II. Carbon dioxide hypersensitivity theory
The researchers found that panic attacks were induced when 5 percent CO2 was inhaled in patients with panic disorder, and that intravenous sodium lactate or sodium bicarbonate had the same effect. It is speculated that the hypersensitivity of CO2 receptors located in the locus coeruleus of the brain stem in the patient causes the patient’s body to alarm for suffocation when inhaling CO2, leading to panic attacks [1].
III. Social psychological theory
Psychosocial factors suggest that panic disorder is caused by the individual’s fear of subconscious impulses affecting real life, or by a conditioned connection formed by a traumatic event in life. But these theories still need scientific confirmation [1].
3. Description of Drugs
3.1. Drugs origin
3.1.1. Fluoxetine. In the 1960s, autopsy studies found that depressed people who were suicidal had reduced serotonin levels, so pharmaceutical companies began investigating serotonin’s role in depression. Among them, Eli Lilly has developed a method that effectively and selectively inhibits serotonin reuptake by the serotonin operator, thereby increasing serotonin concentration in the synaptic cleft. The drug, fluoxetine, was demonstrated by several scientists in 1975 to be an antidepressant and has a weak affinity for the norepinephrine functional protein, which is where fluoxetine differs pharmacologically from other drugs. Fluoxetine was approved by the US Food and Drug Administration in December 1987 and launched in 1988 under the brand name Prozac, selling $3.5 billion a month later and earning $2.6 billion that same year. It has since become a world-famous antidepressant [8].
3.1.2. Alprazolam. Alprazolam belongs to a class of drugs called benzodiazepines, which were first discovered by chemist Leo Sternbach in 1955. This class of drugs appeared to be less toxic, less likely to cause dependence than older drugs, and did not have respiratory depression. This led to a skyrocketing demand for this drug in the 1970s, and it topped the list of “most commonly prescribed drugs” [9]. Alprazolam was first released in 1981 by Upjohn Laboratories (now part of Pfizer) as the first drug approved for the treatment of panic disorder. Although there have been concerns in the medical community about the drug’s addictive nature and its dangers when used in the elderly, Alprazolam is now the most commonly used benzodiazepine in the United States because of its usefulness [10].
3.2. Structure and Synthesis
3.2.1. Fluoxetine
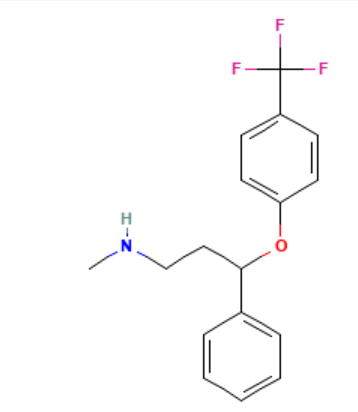
Figure 2. The structure of Fluoxetine
Fluoxetine is an insoluble solid with the structure n-methyl-3-phenyl-3 -[4-(trifluoromethyl) phenoxy] propane-1 amine and the formula C17H18F3NO, an aromatic ether composed of 4-trifluoromethyl phenol, where the hydrogen of the phenol hydroxyl group is replaced by 3-(methylamino) -1-phenylpropyl [11].
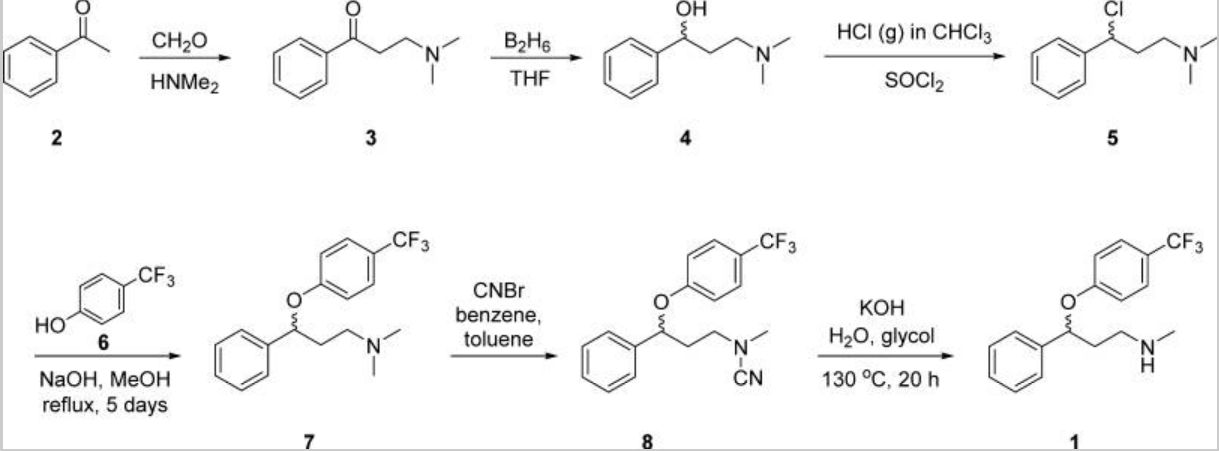
Figure 3. The original synthesis process of fluoxetine
The original synthetic route of fluoxetine (label 1) was reported by Molloy and Schmiegel in 1982 in the United States. Using acetophenone (label 2) as raw material, they obtained β-dimethylaminopropenone oil (label 3) through the Mannich reaction. Dissolve it in tetrahydrofuran and drop it into tetrahydrofuran solution of tetraborane and stir overnight. Then add an equal amount of diborane and stir again overnight. The acid treatment provides the key racemic secondary alcohols (labeled 4). The alcohol is then dissolved in CHCl3 and saturated with anhydrous HCl gas while dropping SO2Cl to maintain reflux for about 5 hours. After the solvent evaporates, the substance labeled 5 in the figure is obtained and collected as crystalline hydrochloride. Then 5 is added to the alkaline solution (label 6) and reflux for 5 days to obtain phenoxyether (label 7). Racemic fluoxetine (label1) is then provided as a free base by an N-cyanide derivative (label 8) and subsequent alkaline hydrolysis [12].
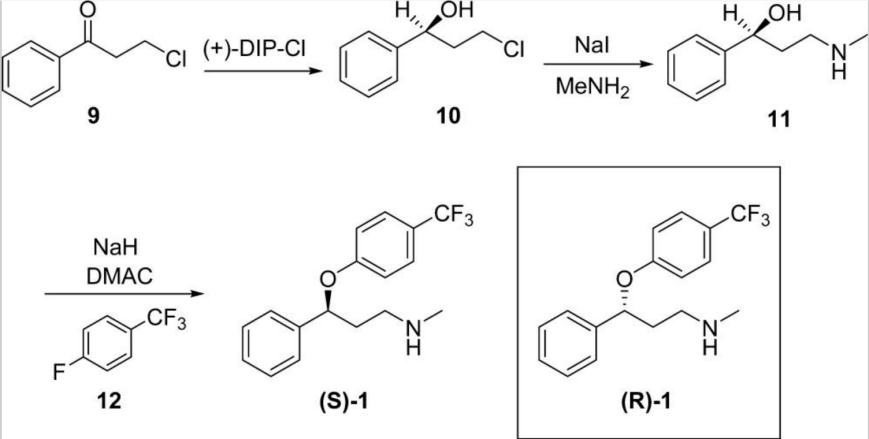
Figure 4. Eli Lily’s method of synthesizing fluoxetine
Eli Lilly’s method of making fluoxetine is to use the Finkelstein reaction to prepare the corresponding iodide in situ, and then replace it with methylamine to obtain the substance labeled 11 in the figure. The material was deprotonated in DMAC with NaH, then 1-fluoro-4 -(trifluoromethyl) benzene (labeled 12) was added, and (S) -fluoxetine (S)-1 was delivered at an S:R ratio of 96:4. Since only (+)-DIP-Cl is available, this asymmetric synthesis allows only (S) -fluoxetine to be obtained. To obtain (R) -fluoxetine (R)-1, Robertson and colleagues employed a classical resolution technique for the d- and L-mandelates of racemate 1. After conversion to the corresponding (R)-1-(1-naphthyl) ethyl urea, HPLC and NMR confirmed that the S:R enantiomer ratio of (S) -fluoxetine (S)-1 was greater than 99:1, and the S:R enantiomer ratio of (R) -fluoxetine (R)-1 was 1.5:98.5 [12].
3.2.2. Alprazolam
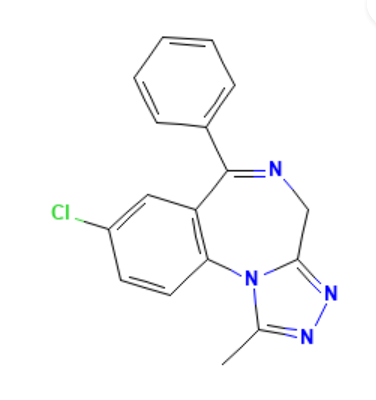
Figure 5. The structure of alprazolam
Alprazolam is a member of the triazolium benzodiazepine class, a 4H-[1,2,4] triazolium [4,3-a][1,4] benzodiazepine class that carries methyl, phenyl, and chlorine substituents at positions 1, 6, and 8, respectively. Alprazolam is only found in people who take the drug [13].
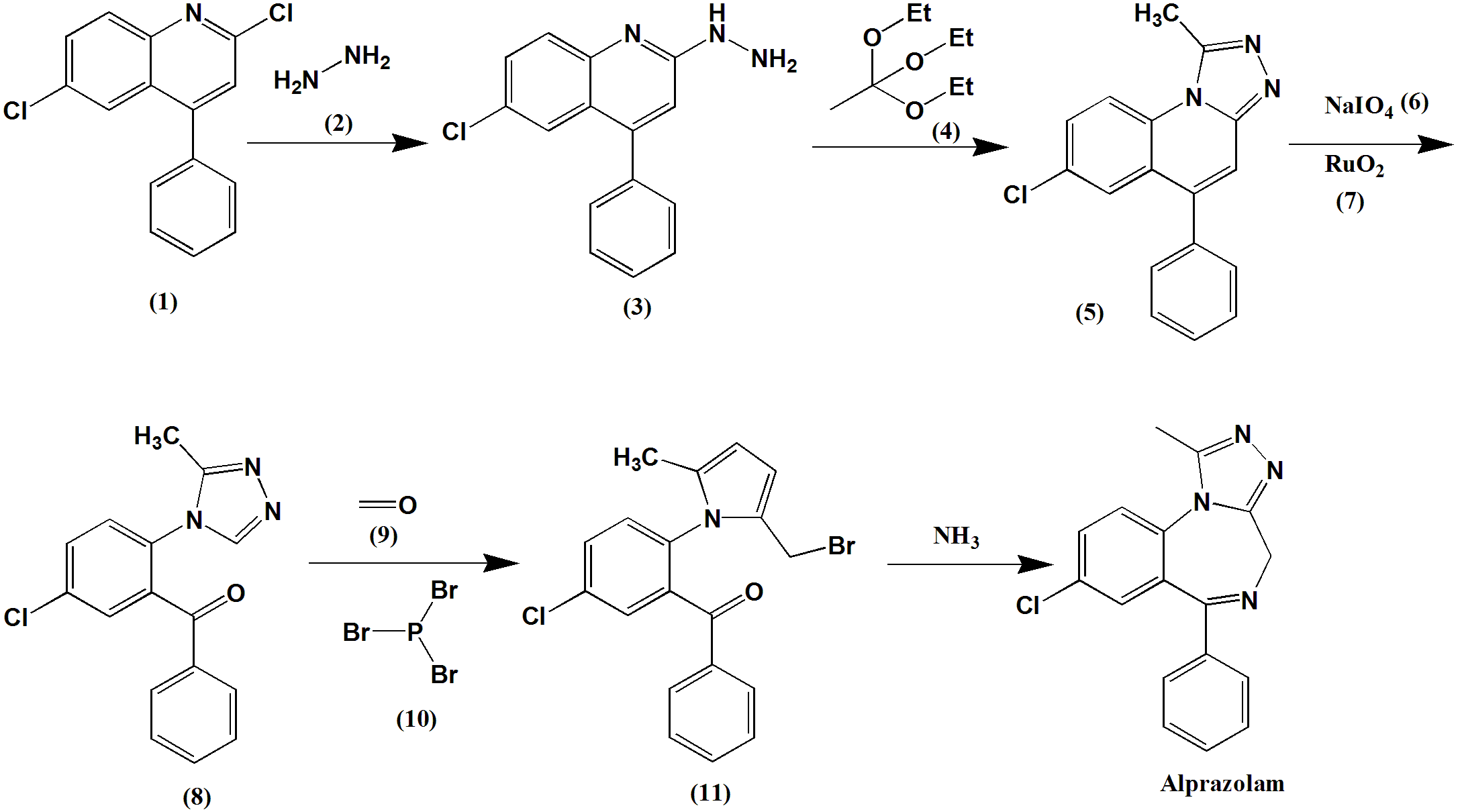
Figure 6. The synthesis of alprazolam
The synthesis of alprazolam is to firstly let 2,6, -dichloro-4-phenylquinoline (label 1) reacts with hydrazine (label 2) to give 6-chloro-2-hydrazine-4-phenylquinoline (label 3). Then, phenylquinoline and triethyl acetate (mark 4) were boiled in xylene to heterocyclic form triazole derivatives (mark 5). 2-[4-(3 ‘-methyl-1,2, 4-triazole)] -5-chlorobenzophenone (8) is produced by oxidative cleavage of sodium periodate (mark 6) and ruthenium dioxide (mark 7) in an acetone-water system. The hydroxyl group is then replaced by phosphorus tribromide (mark 10) to give 2-[4-(3 ‘-methyl-5’ -bromomethyl-1,2, 4-triazole)] -5-chlorobenzophenone (mark 11). Finally, the bromine atom replaces the amino group with ammonia and spontaneously heterocycles to form alprazolam [14].
3.3. Pharmacology
3.3.1. Fluoxetine. Fluoxetine increases serotonin levels by blocking the reabsorption of the presynaptic end working protein and preventing serotonin from being reabsorbed by the body. It is slightly active on both the 5-HT2A receptor in the cerebral cortex and the 5-HT2C receptor in the limbic system, but has little effect on the reuptake of norepinephrine and other neurotransmitters. When the cytochrome P450 enzyme (CYP2D6) acts on fluoxetine, it stimulates its production of the active metabolite norfluoxetine, and precisely because fluoxetine is metabolized on the CYP2D6 isoenzyme, norfluoxetine has several drug interactions. Equally important is that fluoxetine has a half-life of 2 to 4 days and norfluoxetine has a half-life of 7 to 9 days [15]. In treating panic disorder, the researchers conducted two 12-week randomized, multicenter Phase III trials. Data from the first trial showed that 42% of subjects in the fluoxetine treatment group did not have a recurrence after the trial, while this proportion dropped to 28% in the placebo group. In the second trial, 62% of fluoxetine-treated patients did not have panic attacks at the end of the study, compared with 44% of the placebo group [16]. At the same time, in patients who received 10 or 20mg of fluoxetine or placebo, the researchers found that the 20mg daily dose of fluoxetine had the most significant improvement in panic disorder. And they believe that the drug is well tolerated and that its safety in treating panic disorder is about the same as in treating other conditions [17]. These trials strongly demonstrated the effectiveness of fluoxetine in treating panic disorder.
3.3.2. Alprazolam. Alprazolam belongs to a class of drugs known as benzodiazepines. These drugs bind to the GABA-A receptor. This receptor consists of five subunits, and the GABA-A receptor commonly found in the central nervous system consists of two alpha-1 subunits, two beta-2 subunits, and one gamma-2 subunit. Benzodiazepine binding sites are located between the alpha-1 and gamma-2 subunits. A mouse study has shown that alpha-1 subunits mediate the sedative, forgetting, and disordered effects of benzodiazepines, and alpha-2 and alpha-3 subunits mediate the antianxiety and muscle relaxation effects of benzodiazepines. In addition, studies have shown that benzodiazepine-1 receptors affect sedation and anti-anxiety, while benzodiazepine-2 receptors affect muscle relaxation, anti-convulsive activity, memory, and motor coordination. When bound to GABA-A receptors, the main inhibitory neurotransmitter GABA mediates the sedative or inhibitory effects of alprazolam on the human nervous system [18].
One trial suggests that benzodiazepines may have advantages in improving panic symptoms and reducing the number of participants who drop out of treatment. Of the 4,233 participants, 2,124 adults with panic disorder who were treated with benzodiazepines had a lower dropout rate, and the results showed that this class of drugs also had advantages in terms of remission and social function endpoint data [19].
3.3.3. Application. Although both fluoxetine and alprazolam are effective treatments for panic disorder, a combination of the two drugs is most commonly used clinically. In the initial stage, the patient’s symptoms will be significantly improved, and the early adverse reactions of fluoxetine can be alleviated. However, after 4-6 weeks, tolerance may occur and there is no obvious advantage, so it is possible to stop alprazolam at this time to avoid long-term addiction to alprazolam [1].
3.4. Side effects
3.4.1. Fluoxetine. Some patients who take fluoxetine will have nausea, vomiting, dizziness, headache, fatigue, insomnia, anorexia and other adverse symptoms. Patients with liver disease, diabetes, and cardiovascular disease should use fluoxetine with caution [20]. Even though these side effects of fluoxetine are severe, they mostly appear immediately and go away over time, and it is best to change the timing of treatment after the side effects have resolved on their own. Data show that most of these side effects are dose-related, so if the side effects affect the patient too much, the dose can be reduced, and if these symptoms persist, the patient should try to switch to another drug [15].
3.4.2. Alprazolam. According to the National Center for Addiction, some of the main side effects of taking alprazolam may include reduced mental alertness, confusion, memory problems, dizziness, muscle weakness, slurred speech, blurred vision, or increased depression. In addition to these symptoms, patients who regularly take alprazolam are more likely to become dependent on the drug, even under the supervision of a healthcare provider. At the same time, patients taking alprazolam develop resistance, so in order to produce better results, they need to ingest more of the drug. In such cases, patients are more likely to become dependent. When patients become dependent on withdrawal, they often experience intense withdrawal within hours of the first withdrawal. Common underlying withdrawal symptoms include anxiety, insomnia, hallucinations and seizures. When these symptoms become severe, life-threatening symptoms such as mania and depression can develop [21].
3.5. Economics
Table 1. Average price of fluoxetine
10mg | ||
quantity | Per unit | Price |
21 | $0.87 | $18.31 |
28 | $0.67 | $18.71 |
30 | $0.40-$0.99 | $12.01-$29.84 |
60 | $0.23 | $13.75 |
90 | $0.16-0.78 | $14.48-$70.53 |
100 | $0.14-0.77 | $13.28-$77.32 |
Depending on the pharmacy visited by patients, cost of fluoxetine oral capsule 40mg id around $13 for a supply of 30 capsules. The oral solution is around $0.37 per milliliters, $44.76 for 120 milliliters. Image above illustrates the average price of fluoxetine with different quantities from drug.com [22].
Table 2. Average price of alprazolam
0.25mg | ||
quantity | Per unit | Price |
6 | $1.78 | $10.70 |
15 | $0.83 | $12.50 |
30 | $0.52 | $15.49 |
100 | $0.29 | $29.48 |
500 | $0.22 | $109.42 |
1100 | $0.21 | $209.33 |
Depending on the pharmacy visited by patients, the cost of alprazolam oral tablet 0.5 mg is around $11 for a supply of 6 tablets. The oral concentrate is around $3.43 per milliliters and $102.92 for 30 milliliters. Image above illustrates the average price of fluoxetine with different quantities from drug.com [23].
4. Conclusion
It can be concluded that fluoxetine and alprazolam are ideal drugs for the treatment of panic disorder. Fluoxetine inhibits serotonin reuptake and alprazolam inhibits GABA. Although both drugs have negative effects that can sometimes threaten the life of the patient, in general, the two drugs can be effective as long as the patient is monitored timely and the dosage is adjusted. Not only that, the use of two drugs can also play a very good therapeutic effect in the clinical treatment of panic disorder together. Of course, in addition to SSRIs and benzodiazepines, many other antidepressants or anti-anxiety medications such as SNRIs and tricyclic antidepressants are effective for the treatment of panic disorder. Although the mainstream anti-panic disorder drugs on the market are mainly the two mentioned above, with the development of the trend of time, the possibility of more novel and effective drugs in the future is also very large.
References
[1]. Hao, Wei Lu, Lin Li, Tao Liu, Jintong Zhao,Xudong Wang, Gaohua ‘Psychiatry’ People’s Medical Publishing House July 2018 Accessed 18th July 2023
[2]. American Psychiatric Association ‘Diagnostic and Statistical Manual of Mental Disorder, Fifth Edition’ Arlington, VA, American Psychiatric Publishing 2013 Accessed 16th July 2023
[3]. University of Iowa “It’s Greek to Me: Panic” bam.sites.uiowa.edu 20th Mar. 2023 https://bam.sites.uiowa.edu/its-greek-me/panic
[4]. Maudsley, Henry “The Physiology and Pathology of the Mind” Appleton 1867 books.google.com Accessed 20th Jul. 2023 https://books.google.com/books?id=EfY-AAAAYAAJ&vq
[5]. Maudsley, Henry “The Physiology and Pathology of the Mind” Appleton 1867 books.google.com Accessed 20th Jul. 2023 https://books.google.com/books?id=EfY-AAAAYAAJ&vq
[6]. Nardi, Antonio Egidio and Freire, Rafael Christophe R. “The Panic Disorder Concept: a History Perspective” link.springer.com 26th May 2016 https://link.springer.com/chapter/10.1007/978-3-319-12538-1_1
[7]. Na HR, Kang EH, Lee JH, Yu BH. ‘The Genetic Basis of Panic Disorder’ J Korean Med Sci. June 2011 26(6):701-10. doi: 10.3346/jkms.2011.26.6.701. Epub 2011 May 18. PMID: 21655053; PMCID: PMC3102861.
[8]. Hillhouse, Todd M. and Porter, Joseph H. “A Brief History of the Development of Antidepressant Drugs: from Monoamines to Glutamate” www.ncbi.nlm.nih.gov Feb. 2016 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4428540/
[9]. Wick, Jeannette Y. “The History of Benzodiazepines” pubmed.ncbi.nlm.nih.gov 28th Sep. 2013 https://pubmed.ncbi.nlm.nih.gov/24007886/
[10]. Pendleton, James ‘Xanax (Alprazolam)’ www.goodtherapy.org Accessed 30th July 2023 https://www.goodtherapy.org/drugs/xanax-alprazolam.html
[11]. NCBI “Fluoxetine” pubchem.ncbi.nlm.nih.gov Accessed 20th Jul. 2023 https ://pubchem.ncbi.nlm.nih.gov/compound/fluoxetine
[12]. Wenthur CJ, Bennett MR, Lindsley CW. Classics in Chemical Neuroscience: Fluoxetine (Prozac). ACS Chem Neurosci. November 2013 9;5(1):14–23. doi: 10.1021/cn400186j. PMCID: PMC3894728.
[13]. NCBI “Alprazolam” pubchem.ncbi.nlm.nih.gov Accessed 20th Jul. 2023 https ://pubchem. ncbi.nlm.nih.gov/compound/2118
[14]. Huzefakifayet ‘Alprazolam Synthesis, SAR, MCQ, Struecture, Chemical Properties and Therapeutic Uses’ gpatindia.com 13th April 2020 https://gpatindia.com/alprazolam-synthesis-sar-mcqstructurechemical-properties-and-therapeutic-uses/
[15]. Sohel, Ahsan J Shutter, Mollie C Molla, Mohammed ‘Fluoxetine’ www.ncbi.nlm.nih.gov 4th July 2022 https://www.ncbi.nlm.nih.gov/books/NBK459223/
[16]. Wikipedia ‘Fluoxetine’ en.wikipedia.org/ Accessed 20th July 2023 https://en.wikipedia.org/wiki/Fluoxetine#Medical_uses
[17]. Michelson D, Lydiard RB, Pollack MH, Tamura RN, Hoog SL, Tepner R, Demitrack MA, Tollefson GD. ‘Outcome assessment and clinical improvement in panic disorder: evidence from a randomized controlled trial of fluoxetine and placebo. The Fluoxetine Panic Disorder Study Group.’ Am J Psychiatry. November 1998 https://pubmed.ncbi.nlm.nih.gov/9812120/
[18]. George, Tobin T. and Tripp, Jayson “Alprazolam” www.ncbi.nlm.nih.gov 24th Apr. 2023 https://www.ncbi.nlm.nih.gov/books/NBK538165/
[19]. Breilmann, J Girlanda, F Guaiana, G Barbui, C Cipriani, A Castellazzi, M Bighelli, I Davies, SJC Furukawa, TA Koesters, M ‘Benzodiazepines for Panic Disorder in Adults’ www.cochrane.org 28th March 2019 https://www.cochrane.org/CD010677/DEPRESSN_benzodiazepines-panic-disorder-adults
[20]. Yang, Baofeng Chen, Jianguo Zang, Jinwei Wei, Minjie ‘Pharmacology’ People’s Medical Publishing House July 2018
[21]. Walker, Leah K ‘Xanax Abuse: Short-and Long-Term Effects of Xanax’ American addictioncenters.org 3rd July 2023 https://americanaddictioncenters.org/xanax-treatment/ long-term-severe
[22]. Drugs.com ‘Fluoxetine Prices, Coupons and Patient Assistance Programs’ www.drugs.com Accessed 25th July 2023 https://www.drugs.com/price-guide/fluoxetine#oral-capsule-20-mg
[23]. Drugs.com ‘Alprazolam Prices, Coupons and Patients Assistance Programs’ www.drugs.com Accessed 25th July 2023 https://www.drugs.com/price-guide/alprazolam#oral-tablet-0-25-mg
Cite this article
Cheng,C. (2024). Efficiency of fluoxetine and alprazolam in the treatment of panic disorder. Theoretical and Natural Science,46,14-22.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Modern Medicine and Global Health
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Hao, Wei Lu, Lin Li, Tao Liu, Jintong Zhao,Xudong Wang, Gaohua ‘Psychiatry’ People’s Medical Publishing House July 2018 Accessed 18th July 2023
[2]. American Psychiatric Association ‘Diagnostic and Statistical Manual of Mental Disorder, Fifth Edition’ Arlington, VA, American Psychiatric Publishing 2013 Accessed 16th July 2023
[3]. University of Iowa “It’s Greek to Me: Panic” bam.sites.uiowa.edu 20th Mar. 2023 https://bam.sites.uiowa.edu/its-greek-me/panic
[4]. Maudsley, Henry “The Physiology and Pathology of the Mind” Appleton 1867 books.google.com Accessed 20th Jul. 2023 https://books.google.com/books?id=EfY-AAAAYAAJ&vq
[5]. Maudsley, Henry “The Physiology and Pathology of the Mind” Appleton 1867 books.google.com Accessed 20th Jul. 2023 https://books.google.com/books?id=EfY-AAAAYAAJ&vq
[6]. Nardi, Antonio Egidio and Freire, Rafael Christophe R. “The Panic Disorder Concept: a History Perspective” link.springer.com 26th May 2016 https://link.springer.com/chapter/10.1007/978-3-319-12538-1_1
[7]. Na HR, Kang EH, Lee JH, Yu BH. ‘The Genetic Basis of Panic Disorder’ J Korean Med Sci. June 2011 26(6):701-10. doi: 10.3346/jkms.2011.26.6.701. Epub 2011 May 18. PMID: 21655053; PMCID: PMC3102861.
[8]. Hillhouse, Todd M. and Porter, Joseph H. “A Brief History of the Development of Antidepressant Drugs: from Monoamines to Glutamate” www.ncbi.nlm.nih.gov Feb. 2016 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4428540/
[9]. Wick, Jeannette Y. “The History of Benzodiazepines” pubmed.ncbi.nlm.nih.gov 28th Sep. 2013 https://pubmed.ncbi.nlm.nih.gov/24007886/
[10]. Pendleton, James ‘Xanax (Alprazolam)’ www.goodtherapy.org Accessed 30th July 2023 https://www.goodtherapy.org/drugs/xanax-alprazolam.html
[11]. NCBI “Fluoxetine” pubchem.ncbi.nlm.nih.gov Accessed 20th Jul. 2023 https ://pubchem.ncbi.nlm.nih.gov/compound/fluoxetine
[12]. Wenthur CJ, Bennett MR, Lindsley CW. Classics in Chemical Neuroscience: Fluoxetine (Prozac). ACS Chem Neurosci. November 2013 9;5(1):14–23. doi: 10.1021/cn400186j. PMCID: PMC3894728.
[13]. NCBI “Alprazolam” pubchem.ncbi.nlm.nih.gov Accessed 20th Jul. 2023 https ://pubchem. ncbi.nlm.nih.gov/compound/2118
[14]. Huzefakifayet ‘Alprazolam Synthesis, SAR, MCQ, Struecture, Chemical Properties and Therapeutic Uses’ gpatindia.com 13th April 2020 https://gpatindia.com/alprazolam-synthesis-sar-mcqstructurechemical-properties-and-therapeutic-uses/
[15]. Sohel, Ahsan J Shutter, Mollie C Molla, Mohammed ‘Fluoxetine’ www.ncbi.nlm.nih.gov 4th July 2022 https://www.ncbi.nlm.nih.gov/books/NBK459223/
[16]. Wikipedia ‘Fluoxetine’ en.wikipedia.org/ Accessed 20th July 2023 https://en.wikipedia.org/wiki/Fluoxetine#Medical_uses
[17]. Michelson D, Lydiard RB, Pollack MH, Tamura RN, Hoog SL, Tepner R, Demitrack MA, Tollefson GD. ‘Outcome assessment and clinical improvement in panic disorder: evidence from a randomized controlled trial of fluoxetine and placebo. The Fluoxetine Panic Disorder Study Group.’ Am J Psychiatry. November 1998 https://pubmed.ncbi.nlm.nih.gov/9812120/
[18]. George, Tobin T. and Tripp, Jayson “Alprazolam” www.ncbi.nlm.nih.gov 24th Apr. 2023 https://www.ncbi.nlm.nih.gov/books/NBK538165/
[19]. Breilmann, J Girlanda, F Guaiana, G Barbui, C Cipriani, A Castellazzi, M Bighelli, I Davies, SJC Furukawa, TA Koesters, M ‘Benzodiazepines for Panic Disorder in Adults’ www.cochrane.org 28th March 2019 https://www.cochrane.org/CD010677/DEPRESSN_benzodiazepines-panic-disorder-adults
[20]. Yang, Baofeng Chen, Jianguo Zang, Jinwei Wei, Minjie ‘Pharmacology’ People’s Medical Publishing House July 2018
[21]. Walker, Leah K ‘Xanax Abuse: Short-and Long-Term Effects of Xanax’ American addictioncenters.org 3rd July 2023 https://americanaddictioncenters.org/xanax-treatment/ long-term-severe
[22]. Drugs.com ‘Fluoxetine Prices, Coupons and Patient Assistance Programs’ www.drugs.com Accessed 25th July 2023 https://www.drugs.com/price-guide/fluoxetine#oral-capsule-20-mg
[23]. Drugs.com ‘Alprazolam Prices, Coupons and Patients Assistance Programs’ www.drugs.com Accessed 25th July 2023 https://www.drugs.com/price-guide/alprazolam#oral-tablet-0-25-mg