






1. Introduction
The United States healthcare system presents a paradox in the global landscape of medical services, in this paper explores contemporary structures and situations of the American health system.
One of the most significant characteristics of the US healthcare system is its ultimately high-cost burden. Although America is one of the wealthiest nations in the world, the disproportionate amount of its GDP on healthcare still greatly surpasses other developed countries. This high-pressure financial burden not only influences individuals but also exists in entire healthcare infrastructures, which will also impose pressure on governments and healthcare institutions. This setup features publicly financed government programs like Medicare and Medicaid alongside privately financed market coverage through private health insurance plans. The predominant means of financing and delivering healthcare involve out-of-pocket payments and market provision of coverage. As of 2019, approximately 50% of citizens obtained private insurance coverage through their employer (group insurance), while 6% relied on private insurance through health insurance marketplaces (nongroup insurance). Additionally, 20% of citizens were covered by Medicaid, 14% by Medicare, and 1% by other public insurance forms such as the Veterans Health Administration (VHA) and Military Health Service (MHS), leaving 9% of Americans uninsured.[1]
American health spending is expensive. Insanely, outlandishly expensive. They spend $2.8 trillion on health care annually. That works out to about one-sixth of the total economy and more than $8,500 per person — and way more than any other country. On average, Americans see the doctor less than people in other countries.
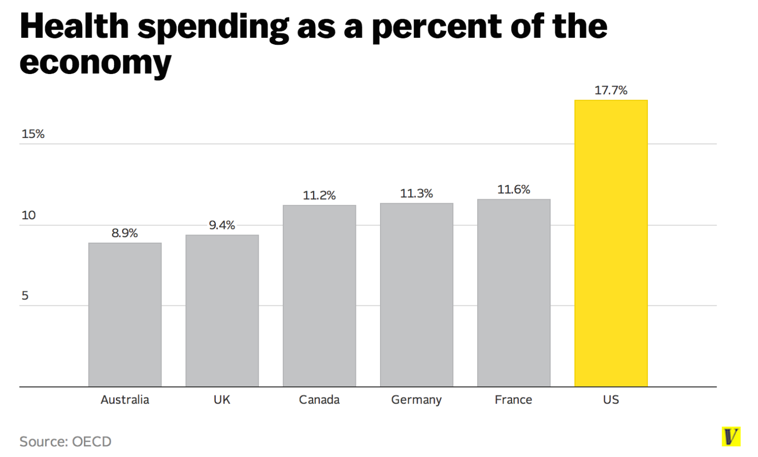
Figure 1. Health spending as a percent of the economy [1]
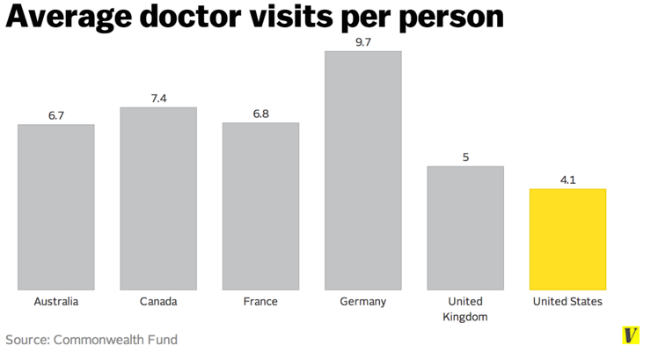
Figure 2. Average doctor visits per person [1]
In America, the cost of healthcare, from prescription medications to imaging scans, tends to be significantly higher compared to other countries. For example, Nexium, a common heartburn medication, costs $215 in the U.S. but only $23 in the Netherlands. This big comparison is mainly due to the lack of price regulation in America. It differs from other nations. In most countries, such as British, the government takes responsibility for negotiating with medical companies, ensuring the low price. Nevertheless, in the United States, individual insurance firms directly set the price with medical companies, therefore, they are hard to gain benefits. This lack of collective bargaining power leads to inflated prices across the board. Some proponents of the American healthcare system argue that this model can stimulate innovation by providing financial incentives for companies to develop groundbreaking drugs and technologies. Somehow, it can gain rationality while it also means Americans have to take on the disproportional burden.
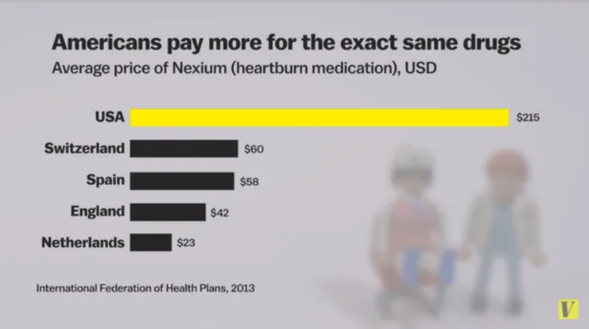
Figure 3. Americans pay more for the exact same drugs[1]
In the healthcare system, it becomes obvious that these challenges are deeply intertwined with broader structural and systemic issues. Factors such as the complex interplay between private and public insurance systems, disparities in access to care based on socio-economic status, and the intricate web of regulations governing healthcare provision all contribute to the complexity of the landscape.
2. Causes
2.1. Fragmented System
Unlike many countries with centralized or single-payer healthcare systems, the United States operates with a fragmented payment structure involving multiple stakeholders such as private insurers, government programs (like Medicare and Medicaid), employers, and individual patients.
In the purely single-payer system, there is merely one single-payer – the government. In many other countries, the government negotiates with medical institutions and covers everyone’s medical expenses. Instead of covering all medical treatment for their residents, many governments opt to pay for most but not all of it. In these countries, individuals have the opportunity to purchase "supplementary" private insurance, which covers services like dental care that are excluded from the government healthcare program. Additionally, people often have the option to buy "complementary" private insurance, which covers co-pays and deductibles in the government's insurance plan.
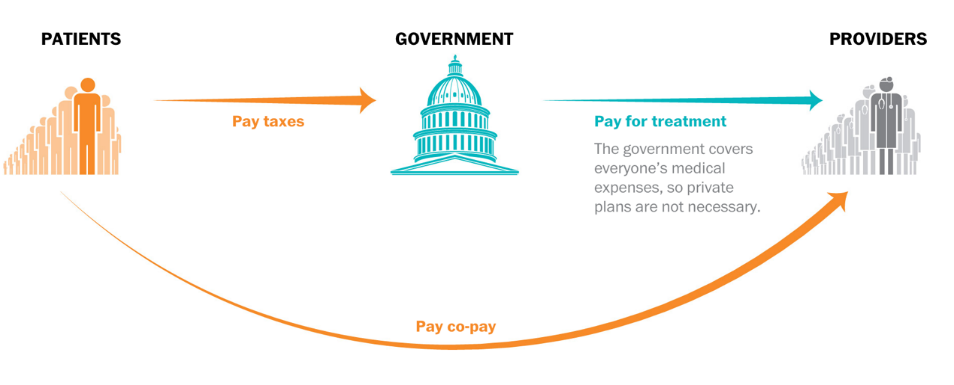
Figure 4. Single-payer systems [2]
The general structure of healthcare systems is similar across the board, but the identity of the payers can differ significantly. In the private insurance market of the United States, patients usually buy coverage from one of many competing insurers. As individuals end up with various insurers, there are multiple payers within the U.S. healthcare system. Sanders' proposal pushes universal coverage to an almost extreme level: Government insurance would encompass numerous services with minimal co-pays, rendering private insurance almost redundant. However, this approach comes with a hefty price tag, estimated at $32 trillion over a decade by the Urban Institute. Such expenditure would represent a significant increase of over 50 percent in federal spending, as projected by the Congressional Budget Office. While the elimination of premiums to private insurers could partially offset this cost, the government's monopoly might enable the implementation of cost-saving measures.
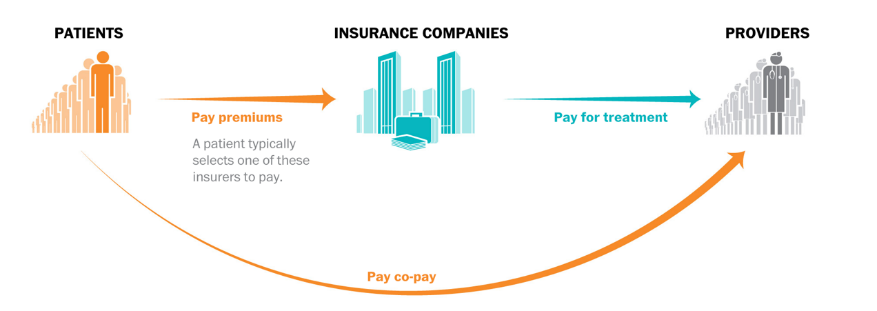
Figure 5. Insurance market [2]
Under fragmented management, inefficiency, costs of management and complexity of negotiation result in the American healthcare system and push high costs. Thus, the general prices of American prescription medicines always be much higher than other nations. American medical firms usually have more freedom in setting prices. In addition, long-term patents monopoly the markets and maintain the monopoly power for these firms. Low competition eventually leads to high prices.
2.2. Market Dynamics
The healthcare market in the US operates under a predominantly for-profit model. Hospitals, pharmaceutical companies, and insurance providers seek to maximize revenue and shareholder returns. This profit-driven approach can lead to inflated prices for medical services, drugs, and insurance premiums as stakeholders prioritize financial gains over cost containment or affordability for patients. In 1987 private insurance firms in the United States retained $18.7 billion for administration and profits out of total premium revenues of $157.8 billion. [3] Their average overhead costs (11.9 percent of premiums) were considerably higher than the 3.2 percent administrative costs of government health programs such as Medicare and Medicaid ($6.6 billion out of total expenditures of $207.3 billion). Together, the administration of private and public insurance programs consumed 5.1 percent of the $500.3 billion spent on health care, or $106 per capital [3].
2.3. Administrative Costs
Compared to other nations, US healthcare system management costs are ultimately high. Except for those factors this paper mentioned before, the complex accounting process, large amount of transcript works and healthy insurance providers' need to consider different ranges and rates of returns in insurance all lead to financial burdens for governments and insurance institutions. As a result, firms always want to transfer the costs to consumers, therefore pushing the prices.
The United States is one of the most expensive countries in the healthcare market all over the world. In 2022, healthcare spending in the U.S. soared to $4.5 trillion, averaging $13,493 per person. This figure stands in stark contrast to the average cost per person in other affluent nations, which is less than half as much. Despite the COVID-19 pandemic exacerbating the trend of rising healthcare costs, such expenditures have been on the rise long before the onset of COVID-19. Over the past few decades, healthcare costs relative to the size of the economy have surged, climbing from 5 percent of GDP in 1962 to 17 percent in 2022. [4]
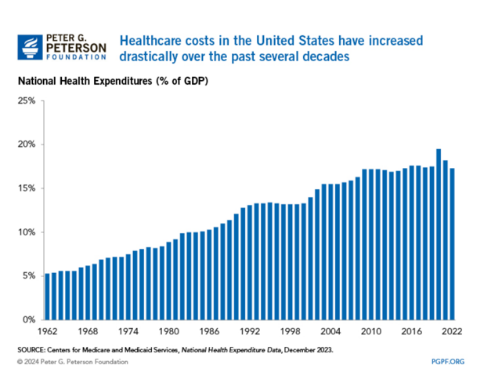
Figure 6. Healthcare costs in the United States have increased drastically over the past several decades [4]
3. Potential Solutions
3.1. Price Regulation and Negotiation
Price regulation needs government interventions and other institutions, such as the Food and Drug Administration (FDA) or the Centers for Medicare & Medicaid Services (CMS). These institutions can establish guidelines or regulations to manage the functions of drug price setting. One approach to impose a price ceiling which is lower than the market equilibrium price, preventing pharmaceutical companies from charging excessively high prices for essential medications. The price of price ceiling can be considered by factors such as the cost of production and the quantity demanded of the drugs. Moreover, the government can directly imitate the price of the same drugs in other nations. In addition, governments can also negotiate directly with pharmaceutical companies to ask for lower prices. They can get special discount for large amount of quantity demanded of drugs in American medicine markets. However, as this paper mentioned before, it may be not justifiable for America due to the specific structure in America.
The Department of Health and Human Services (DHHS) is the primary institution for federal healthcare regulatory activity in the United States. As a sprawling organization, DHHS commands considerable resources and influence within the federal government. In 2005, its budget of $581 billion accounted for nearly a quarter of all federal spending, trailing only the Department of Defense in terms of budgetary allocation among cabinet-level agencies. With a workforce of 67,444 employees, DHHS oversees a vast array of responsibilities, managing over 300 distinct programs and administering more grant funding than all other federal agencies combined.[5]
3.2. Enhancing Price Transparency and Consumer Empowerment
On one hand, price transparency can promote the understanding of patients and consumers. It includes the costs of medical services, operations and medications, helping patients willing to estimate the cost and decide the program. It is beneficial for patients to know their financial responsibilities and predict the costs of treatment, reducing the accidents costs and risks imposed on patients.
The public policy objective of promoting price transparency in medical care began to take shape during the presidency of George W. Bush, particularly in support of consumer-driven healthcare initiatives. A notable policy achievement of this administration was the introduction of Health Savings Accounts (HSAs), which were made available to all private insurance contracts as long as they were paired with a high-deductible health plan (HDHP).[5]
Since their inception in the early 2000s, HSAs and HDHPs have experienced significant growth, evolving from a relatively small portion of the health insurance market to becoming one of the fastest-growing health plan designs by 2021. They have become the second most preferred health insurance design, trailing only Preferred Provider Organizations (PPOs) in popularity among employers.
3.3. Streaming Administrative Processes
Implementing standardized coding systems, such as Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) codes, ensures accurate and consistent billing costs for healthcare providers and payers. Standardized codes streamline the claims submission process, reducing errors and delays in reimbursement. Adopting interoperable HER (electronic health records) systems enables healthcare providers to digitize patient records, streamline documentation, and eliminate paper-based workflows. EHRs improve data accuracy, accessibility, and sharing among healthcare providers, enhancing care coordination and reducing administrative burdens associated with paper-based record-keeping. Automating routine administrative tasks, such as appointment scheduling, eligibility verification, and prior authorization processes, minimizes manual intervention and streamlines workflow efficiency. Automated systems utilize software algorithms and decision support tools to expedite administrative processes and reduce processing times.
In 1946, Congress introduced the Administrative Procedures Act (APA) to ensure that federal regulatory proceedings adhere to Constitutional due process. This landmark legislation provides a framework for administrative decision-making, serving as a guide for regulatory agencies. Many states have enacted similar laws to govern their regulatory programs.
The application of the APA's principles can vary depending on the type of proceeding involved. However, certain fundamental elements remain consistent. One such principle is the requirement that administrative decisions must not be deemed "arbitrary, capricious, an abuse of discretion, or otherwise not by the law." This standard serves as a common benchmark for evaluating the validity of administrative actions under the APA.
4. Implications for various stakeholders
4.1. Drug Price Regulation and Negotiation
Regulation and negotiation of drug prices can lower the costs for patients of drugs, enhancing the affordability and opportunities to get fundamental treatments. Thus, it can help reduce the financial burden for patients and increase the addiction of drugs. However, lowering prices also has drawbacks. It will reduce the innovation and motivation of firms. Many medical companies need to change their strategies which can lower their roots costs therefore still maintaining the profits to ensure their competitive power. Generally, when government sets the basic price for the markets, balancing providers and consumers should be seriously considered. To some extent, regulations need to be cooperated with related industries which can get benefits from US healthcare industry, and consider the potential impacts.
4.2. Price Transparency and Consumer Empowerment
As this paper mentioned before, promoting price transparency can help patients to make rational choices, avoiding high-risk burdens and potential bills. Because patients can reduce the price of bills by their own willingness, which enhance the satisfaction of the healthcare system. Providers of the healthcare insurance need to calculate the costs of promoting transparency, ensuring the quality of this policy. Somehow, this policy might slight increase the costs of healthcare insurance, as calculation and labor force are increasing. However, this is still essential because it will be the base for the government to cut the high prices.
The projected impact of price transparency is anticipated to vary greatly based on regional differences and income levels. Nationally, estimates range from $17.6 billion to $80.7 billion in potential savings. [6]
The Midwest region is expected to experience the most significant impact, with a potential savings of $20 billion and an 8% reduction in medical expenditure. Conversely, the South is projected to have the lowest impact, with only a 5.8% reduction. [7]
4.3. Single-Payer Healthcare System
A single-payer system could simplify healthcare access and reduce out-of-pocket expenses for patients by eliminating premiums, deductibles, and copayments. Patients can enjoy the continuity of healthcare and gain more opportunities. It is not only beneficial for consumers, but also for healthcare insurance providers as a single-payer healthcare system can reduce the total costs for them. However, they may also face changes in reimbursement rates and care delivery models, requiring adaptation to new payment structures. Implementing a single-payer system would require significant policy changes and government oversight. Thus, governments and policymakers pay essential roles because they need to balance the political and financial pressure, insuring the equality in the society.
5. Conclusion
In summary, this paper provides a comprehensive view of the American healthcare system, emphasizing its complexities and underlying challenges. The US healthcare system’s high healthcare costs compared to all other developed nations due to staggering cost burdens, fragmented structure, and lack of price controls. To some extent, it can motivate innovation and investments in the market. However, the negative pressures posted on individuals, families, insurance companies and governments are countless. Moving forward, improvements can be made in several areas. Future research should focus on exploring innovative approaches to address the root causes of high healthcare costs, such as implementing effective price regulation mechanisms and streamlining administrative processes. Additionally, enhancing transparency in pricing and empowering consumers to make informed healthcare decisions are essential steps towards promoting affordability and accessibility in the healthcare market.
Furthermore, this paper acknowledges its limitations. Although it provides a comprehensive overview of the current landscape, further research could delve deeper into specific aspects of the healthcare system, such as the impact of policy reforms on healthcare outcomes or the role of technology in driving efficiency and cost containment. Further researches still need to be done. For some kinds of policies, the extent of policy regulations is uncertain, therefore more accurate calculations need to be considered in future developments. By addressing these gaps and embracing innovative solutions, we can strive towards building a more equitable, efficient, and accessible healthcare system for the benefit of all.
References
[1]. Sarah Kliff,8 facts that explain what’s wrong with American health system, https://www.vox.com/2014/9/2/6089693/health-care-facts-whats-wrong-american-insurance
[2]. Kim Soffen, Single-payer would drastically change health care in America, https://www.washingtonpost.com/graphics/2017/national/single-payer-explainer/
[3]. David M. Cutler, Your money or your life, Oxford University Press, Inc.198 Madison Avenue, New York, New York 10016,2004
[4]. Peter G. Peterson Foundation, why Americans paying more for healthcare, https://www.pgpf.org/blog/2024/01/why-are-americans-paying-more-for-healthcare
[5]. Robert I. Field, Health Care Regulation in America: Complexity, Confrontation, and Compromise, Published by Oxford University Press, Inc.198 Madison Avenue, New York, New York 10016, 2007
[6]. Parente ST, Feldman R, Sandy L. Does transparency matter? The impact of provider qualityand cost information on health care cost and preventive services use. ] Health Med Econ.2019:05(01):3.
[7]. Employer Health Benefits Survey. Kaiser family foundation. 2021. Accessed August 28, 2022. https://www.kff.org/report-section/ehbs-2021-summary-of-findings/
[8]. Stephen T. Parente, PhD, Estimating the Impact of New Health Price Transparency Policies, First published online February 17, 2023, https://doi.org/10.1177/00469580231155988
[9]. Steven H. Woolf and Laudan Aron, U.S. Health in International Perspective, national research council and institute of medicine of the national academics
[10]. Alan M. Gaber and Jonathan Skinner, Is American Health Care Uniquely Inefficient, Journal of Economic Perspectives- volume 22, Number 4- Fall 2008- Page 27-50
[11]. Steffie Woolhandler, M.D., M.P.H, and David U. Himmelstein, M.D., The Deteriorating Administrative Efficiency of the U.S Health Care System, Published May 2,1991, DOI:10.1056/NEJM199105023241805
[12]. Adam Gaffney, Danny McCormick, The Affordable Care Act: implications for health-care equity, 2017 Apr8;389(1007):1442-1452. doi:10.1016/S0140-6736(17)30786-9
[13]. Neil Baum, Rules and Incentives: The Problem with American Healthcare, J Med Pract Manage.2015 Jan-Feb;30(4):267-8
Cite this article
Ji,S. (2024). American health system problems and potential solutions . Theoretical and Natural Science,58,89-96.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Biological Engineering and Medical Science
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Sarah Kliff,8 facts that explain what’s wrong with American health system, https://www.vox.com/2014/9/2/6089693/health-care-facts-whats-wrong-american-insurance
[2]. Kim Soffen, Single-payer would drastically change health care in America, https://www.washingtonpost.com/graphics/2017/national/single-payer-explainer/
[3]. David M. Cutler, Your money or your life, Oxford University Press, Inc.198 Madison Avenue, New York, New York 10016,2004
[4]. Peter G. Peterson Foundation, why Americans paying more for healthcare, https://www.pgpf.org/blog/2024/01/why-are-americans-paying-more-for-healthcare
[5]. Robert I. Field, Health Care Regulation in America: Complexity, Confrontation, and Compromise, Published by Oxford University Press, Inc.198 Madison Avenue, New York, New York 10016, 2007
[6]. Parente ST, Feldman R, Sandy L. Does transparency matter? The impact of provider qualityand cost information on health care cost and preventive services use. ] Health Med Econ.2019:05(01):3.
[7]. Employer Health Benefits Survey. Kaiser family foundation. 2021. Accessed August 28, 2022. https://www.kff.org/report-section/ehbs-2021-summary-of-findings/
[8]. Stephen T. Parente, PhD, Estimating the Impact of New Health Price Transparency Policies, First published online February 17, 2023, https://doi.org/10.1177/00469580231155988
[9]. Steven H. Woolf and Laudan Aron, U.S. Health in International Perspective, national research council and institute of medicine of the national academics
[10]. Alan M. Gaber and Jonathan Skinner, Is American Health Care Uniquely Inefficient, Journal of Economic Perspectives- volume 22, Number 4- Fall 2008- Page 27-50
[11]. Steffie Woolhandler, M.D., M.P.H, and David U. Himmelstein, M.D., The Deteriorating Administrative Efficiency of the U.S Health Care System, Published May 2,1991, DOI:10.1056/NEJM199105023241805
[12]. Adam Gaffney, Danny McCormick, The Affordable Care Act: implications for health-care equity, 2017 Apr8;389(1007):1442-1452. doi:10.1016/S0140-6736(17)30786-9
[13]. Neil Baum, Rules and Incentives: The Problem with American Healthcare, J Med Pract Manage.2015 Jan-Feb;30(4):267-8