






1. Introduction
Coronary heart disease is a disease in which the arteries of the heart are unable to deliver enough oxygen-rich blood to the heart, often leading to further cardiac complications and sometimes even death [1]. Cholesterol deposits in the heart arteries and inflammation are the common causes of coronary heart disease. Coronary heart disease typically develops over decades, remaining hidden until suddenly triggering a significant blockage or a heart attack. Unfortunately, it is the most common type of heart disease, with around 697,000 succumbing to the disease and around 18.2 million Americans living with it every year.
Due to the rise in coronary heart disease deaths, many studies have begun to examine the different causes and prevention methods against coronary heart disease, some examining women and others examining men. However, few studies have investigated the differences between men and women when it comes to the risks of coronary heart disease. Therefore, this study intends to discover those differences and provide a base on which medical professionals can continue to build their understanding of the risks of coronary heart disease and provide their patients, whether male or female, with the right advice.
2. Literature review
Many studies have examined the overall risk for both men and women, with a more recent study, based on the Framingham Heart Study [2][3] concluding that cigarette smoking, blood pressure, and cholesterol levels were the most prominent risk factors for coronary heart disease [4]. Previously, some studies had even turned toward dietary factors as causes of coronary heart disease [5].
Despite coronary heart disease being the leading cause of death for women in America, physicians and other medical professionals continue to overlook the risk factors and symptoms of the disease, resulting in later diagnosis and, therefore a higher risk of further complications. As a result, many studies began turning to focus just on women; however, rather than focusing on the common causes, like smoking or a medical history of stroke or diabetes, they centered around female-specific risk factors like hormonal dysfunction and different diseases during pregnancy [6], as well as factors of interest to women [7]. Some studies also turned toward men-specific risk factors, bringing psychological factors into consideration [8].
Additionally, some studies specifically focused on the causes of coronary artery disease rather than coronary heart disease in women [9], which examined factors like age, weight, etc. Many studies have even acknowledged the preventability of coronary heart disease, though regarding gender-specific risk factors [10-12]. Despite all the gender-specific causes examined in previous studies, it is necessary to focus on the plain and straightforward risk factors between men and women mentioned in the above paper, like age, weight, as well as smoking, total cholesterol, blood pressure, and more. Thus, this study aims to examine the significance of each of the common risk factors in both genders, to help physicians easily recognize the presentation and predict the possibility of coronary heart disease, no matter the gender.
3. Methodology
This study will be using data from the Framingham Heart Study. The Framingham Heart Study was launched in 1948 to identify common factors that contribute to cardiovascular diseases [13][14]. The study was inclusive of both genders and occurred across multiple generations, making it the most suitable to examine the effects of various factors on the development of coronary heart disease.
3.1. Study population
The data was first collected in 1948 when an original cohort of 5209 men and women between 30 and 62 years old were recruited from Framingham, Massachusetts. The data from the Framingham Heart Study included biological specimens, molecular genetic data, phenotype data, samples, images, participant vascular functioning data, physiological data, demographic data, and ECG.
The requirements for the initial cohort were an age between 28 and 62 years at the time of the first examination, with no history of heart attack or stroke. Since then, examination data has grown to include 32 clinical exams, selected ancillary data, and event follow-up through 2018. The female participants tended to be older, have a higher education, did not smoke as much, and overall had a lower BMI distribution compared to the males. All the participants in the study will be anonymous. No names of participants or universities will appear in the study.
3.2. Observed characteristics
The data from the Framingham Heart Study takes into consideration several factors to determine a patient’s chance of developing coronary heart disease in the following ten years: gender, age, education, history of smoking, how many packs of cigarettes a participant smokes in a day, whether the participant is on blood pressure medication, previous history of stroke, previous history of hypertension, diagnosis of diabetes, total cholesterol systolic blood pressure, diastolic blood pressure, body mass index, heart rate, and glucose levels. Participants in the Framingham Heart Study along with their children would voluntarily consent to undergo a detailed medical history, physical examination, and medical tests every three to five years.
3.3. Statistical analysis
A regression analysis will be performed on the quantitative data to ultimately determine the most significant risk factors in women and men. Exploratory data analysis will also be performed, providing a visual representation of the various risk factors. Histograms, density plots, scatter plots, box plots, and other tools will be used.
As the regression analysis is carried out, 4 key values emerge--Estimate, Std. Error, and t-value, and P-value. The Estimate is a unique coefficient on each of the parameters examined in the study. The Std. Error, also known as the standard error of the estimate, represents the average distance between observed values and the regression line, indicating the variability of the estimate. The t-value is a measure of how many standard errors a coefficient is away from 0. The larger the t-value, the more evidence there is that there is a significant difference. Lastly, the p-value represents the probability of obtaining the observed result. Therefore, the smaller the p-value, the greater the statistical significance of the observed difference.
The p-value of each variable holds the greatest importance in this study, as it will be used to determine the major factors influencing the development of coronary heart disease in the following ten years of the Framingham Heart Study.
4. Results
In the original cohort of 5209 participants, 644 of them ended up getting coronary heart disease in the following 10 years.
Percent That Got a CHD |
| Percent That Got a CHD |
|
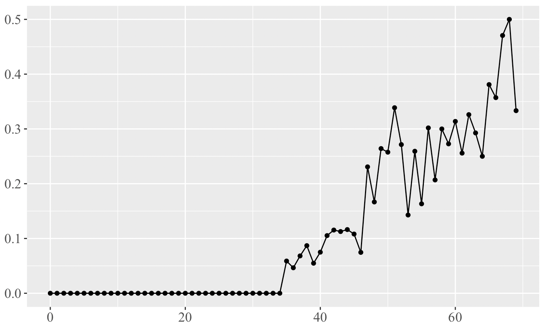
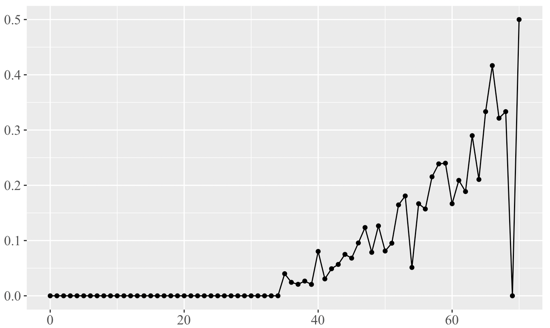
Age | Age | ||
Figure 1. Examines the effect of age on the percentage of men who develop coronary heart disease in the following 10 years. | Figure 2. Examines the effect of age on the percentage of women who develop coronary heart disease in the following 10 years. | ||
Density |
| Density |
|
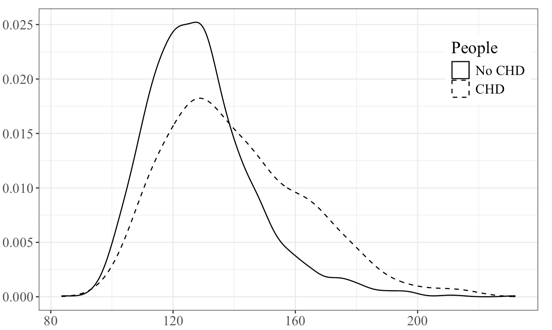
Systolic Blood Pressure | Systolic Blood Pressure | ||
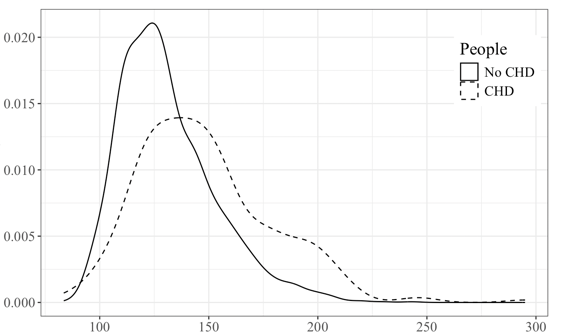
Figure 3. Compares the distribution of systolic blood pressure for men who developed and did not develop coronary heart disease in the following 10 years. | Figure 4. Compares the distribution of systolic blood pressure for women who developed and did not develop coronary heart disease in the following 10 years. | ||
Density |
| Density |
|
Glucose | Glucose | ||
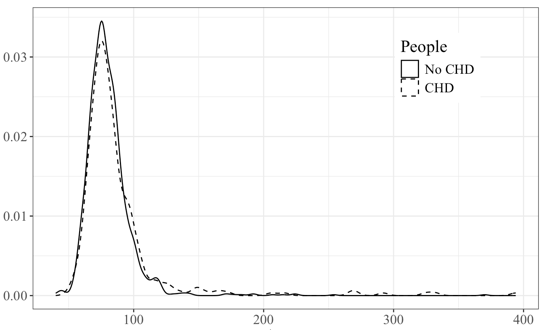
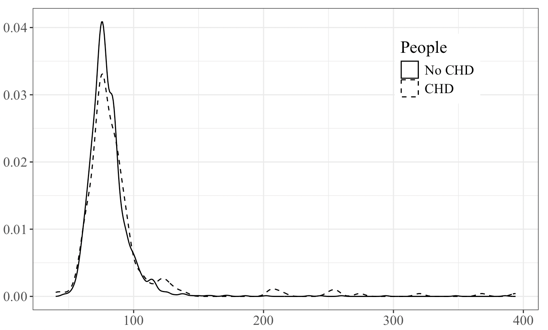
Figure 5. Compares the distribution of glucose levels for men who developed and did not develop coronary heart disease in the following 10 years. | Figure 6. Compares the distribution of glucose levels for women who developed and did not develop coronary heart disease in the following 10 years. | ||
Density |
| Percent That Got a CHD |
|
Total Cholesterol | Cigarettes Per Day | ||
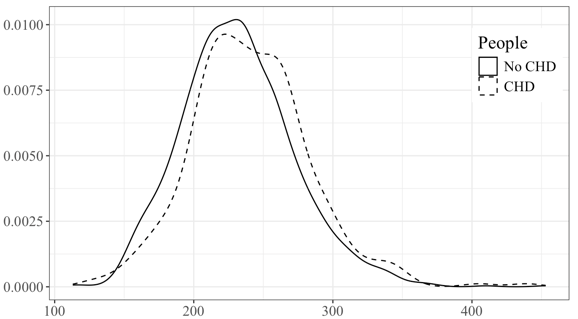
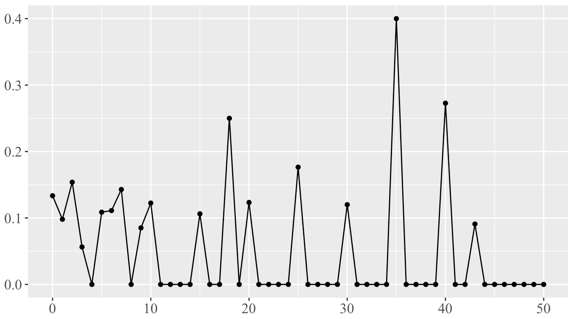
Figure 7. Compares the distribution of total cholesterol levels for men who developed and did not develop coronary heart disease in the following 10 years. | Figure 8. Examines the effect of the number of cigarettes smoked a day on the percentage of women who develop coronary heart disease in the following 10 years. | ||
Count |
|
History of Hypertension | |
Figure 9. Examines the correlation between a history of hypertension and the development of coronary heart disease in women. | |
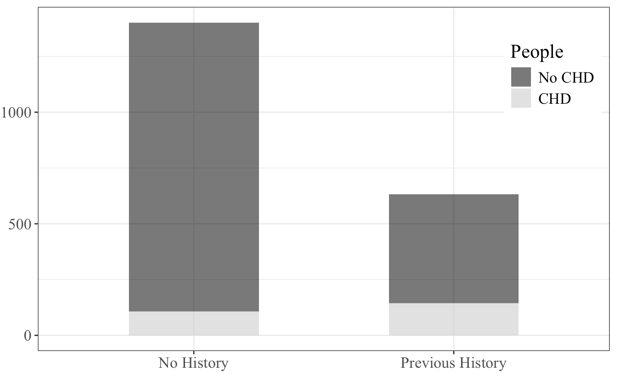
Figures 1, 2, 3, 4, 5, 6, 7, 8, and 9 show the distribution of the important factors when accounting for the risk of coronary heart disease in the following 10 years.
Table 1. Examines male data and presents the coefficients of each variable and the p-value, which illustrates the significance of the variable.
Estimate | Std. Error | t value | Pr(>|t|) | Significancea | |
(Intercept) | -0.9009998 | 0.1401205 | -6.43 | 1.68E-10 | *** |
age | 0.0087684 | 0.0011752 | 7.461 | 1.40E-13 | *** |
Education | 0.0022255 | 0.0086529 | 0.257 | 0.7971 | |
currentSmoker | 0.0243506 | 0.0312592 | 0.779 | 0.4361 | |
cigsPerDay | 0.0017454 | 0.0011031 | 1.582 | 0.1138 | |
BPMeds | 0.0488325 | 0.0681159 | 0.717 | 0.4735 | |
prevalentStroke | 0.1752958 | 0.1252141 | 1.4 | 0.1617 | |
prevalentHyp | 0.0029292 | 0.0274097 | 0.107 | 0.9149 | |
Diabetes | 0.0631861 | 0.0699856 | 0.903 | 0.3667 | |
totChol | 0.000509 | 0.0002287 | 2.226 | 0.0262 | * |
sysBP | 0.0039236 | 0.0008675 | 4.523 | 6.55E-06 | *** |
diaBP | -0.001107 | 0.0013649 | -0.811 | 0.4175 | |
BMI | -0.0007893 | 0.0029427 | -0.268 | 0.7886 | |
heartrate | -0.000137 | 0.0008361 | -0.164 | 0.8699 | |
Glucose | 0.0012195 | 0.0004885 | 2.497 | 0.0126 | * |
a * P ≤ 0.05
** P < 0.01
*** P < 0.001
Table 2. Examines female data and presents the coefficients of each variable and the p-value, which illustrates the significance of the variable.
Estimate | Std. Error | t value | Pr(>|t|) | Significancea | |
(Intercept) | -0.362 | 0.0937 | -3.864 | 0.000115 | *** |
age | 0.00579 | 0.00104 | 5.581 | 2.71E-08 | *** |
education | -0.0121 | 0.00751 | -1.606 | 0.108361 | |
currentSmoker | -0.0132 | 0.0229 | -0.575 | 0.565319 | |
cigsPerDay | 0.00306 | 0.00127 | 2.416 | 0.015796 | * |
BPMeds | 0.0516 | 0.0386 | 1.337 | 0.181227 | |
prevalentStroke | 0.102 | 0.0919 | 1.109 | 0.2675 | |
prevalentHyp | 0.0459 | 0.0225 | 2.044 | 0.041087 | * |
diabetes | -0.0151 | 0.0563 | -0.269 | 0.788175 | |
totChol | -0.00000281 | 0.000168 | -0.017 | 0.986674 | |
sysBP | 0.00186 | 0.000592 | 3.147 | 0.001671 | ** |
diaBP | -0.00154 | 0.000996 | -1.543 | 0.12301 | |
BMI | 0.00131 | 0.00176 | 0.742 | 0.458417 | |
heartRate | -0.000702 | 0.000593 | -1.184 | 0.236654 | |
glucose | 0.00113 | 0.000377 | 2.988 | 0.002844 | ** |
Table 3. Examines male data and presents the variables remaining after variable selection, in which less significant variables were not considered.
Estimate | Std. Error | t value | Pr(>|t|) | Significancea | |
(Intercept) | -0.9794308 | 0.0908595 | -10.78 | < 2E-16 | *** |
age | 0.0090386 | 0.0011314 | 7.989 | 2.56E-15 | *** |
cigsPerDay | 0.0024223 | 0.000681 | 3.557 | 0.000386 | *** |
prevalentStroke | 0.1806188 | 0.1243671 | 1.452 | 0.146611 | |
totChol | 0.0004829 | 0.0002261 | 2.136 | 0.032819 | * |
sysBP | 0.0034653 | 0.0004936 | 7.02 | 3.25E-12 | *** |
Glucose | 0.001486 | 0.0003817 | 3.893 | 0.000103 | *** |
Table 4. Examines female data and presents the variables remaining after variable selection, in which less significant variables were not considered.
Estimate | Std. Error | t value | Pr(>|t|) | Significancea | |
(Intercept) | -0.3881103 | 0.076398 | -5.08 | 4.12E-07 | *** |
age | 0.005937 | 0.0009665 | 6.143 | 9.75E-10 | *** |
education | -0.0131958 | 0.0073396 | -1.798 | 0.072344 | |
cigsPerDay | 0.0023479 | 0.0008204 | 2.862 | 0.004256 | ** |
BPMeds | 0.0593752 | 0.0382122 | 1.554 | 0.120382 | |
prevalentHyp | 0.0469075 | 0.0223505 | 2.099 | 0.035965 | * |
sysBP | 0.0018241 | 0.0005903 | 3.09 | 0.002029 | ** |
diaBP | -0.0014252 | 0.0009702 | -1.469 | 0.14198 | |
glucose | 0.0010524 | 0.0003013 | 3.492 | 0.000489 | *** |
Variables that were not significant before variable selection, but are after, are likely only significant due to the presence of other variables. Tables 1 and 2 show the true individual significance of a variable, while Tables 3 and 4 consider all the variables together and then determine the significance of the variables.
5. Discussion
Our results demonstrated the significance of each variable: gender, age, education, smoking, history of stroke or hypertension, diabetes, cholesterol levels, systolic and diastolic blood pressure, BMI, heart rate, and glucose levels. From analyzing Table 1, it is visible that age, total cholesterol, systolic blood pressure, and glucose are the most significant in determining the risk of coronary heart disease in the following 10 years in men, with age and systolic blood pressure having p-values lower than 0.001. Based on the exploratory data analysis performed, as age, systolic blood pressure, and levels of cholesterol and glucose increased, there was a greater percentage of individuals who developed coronary heart disease in the following ten years.
Similarly, a close analysis of Table 2 shows that age, systolic blood pressure, and glucose are also significant variables in women; however, the number of cigarettes smoked per day and previous history of hypertension are unique significant variables to women. Despite the females in the Framingham Heart Study having a lower percentage of smokers, the number of cigarettes smoked per day by the smokers still has a notable impact on the risk of coronary heart disease. Graphs from the exploratory data analysis support findings from Tables 1 and 2, showing that a previous history of hypertension exists and increased age, systolic blood pressure, glucose levels, and the number of cigarettes smoked per day are associated with a rise in the percentage of individuals who developed coronary heart disease in the following ten years.
The difference in significant factors between males and females that lead to a risk of coronary heart disease is essential to helping medical professionals and others in the field of medicine to be aware of distinct factors that could easily help lead to early diagnosis and treatment. Early diagnosis and treatment are essential in cardiac cases, as each passing minute after a heart attack leads to more of the heart being deprived of oxygen, damage that is often irreversible. Getting diagnosed fast and starting a treatment plan will almost always lead to a better prognosis for the patient. The key to all of this is fully understanding the various factors that lead to a higher risk of coronary heart disease for both genders, which has been determined by this study as seen in the results.
Though the data in this study, which was collected by the Framingham Heart Study, seems well-rounded and gathered well, an explicit limitation emerges. All participants in the first cohort and later cohorts of the Framingham Heart Study were Caucasian, so the data failed to fully represent other races and ethnicities [15]. Though the Framingham Heart Study has provided a solid basis for discovering new knowledge about coronary heart disease, future studies can build on the limitations of the Framingham Heart Study and focus on a variety of races, rather than just Caucasians.
6. Conclusion
This study addresses the different significant aspects between men and women when examining possible causes for an increased risk of coronary heart disease. It illustrates the differences between the critical factors men and women hold and encourages physicians and others in the medical field to be knowledgeable about these differences and use them to provide better medical opinions and advice to patients.
This study also calls for future studies to incorporate different races and ethnicities when investigating the differences in coronary heart disease risks between men and women, allowing for more inclusive standards when it comes to coronary heart disease or other cardiac diseases.
References
[1]. Sanchis-Gomar F, Perez-Quilis C, Leischik R, and Lucia A 2016 Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 4(13):256.
[2]. Kannel WB 1990 Bishop lecture. Contribution of the Framingham Study to preventive cardiology. 15(1):206-11
[3]. Mahmood SS, Levy D, Vasan RS, and Wang TJ 2014 The Framingham Heart Study and the Epidemiology of Cardiovascular Diseases: A Historical Perspective. Lancet. 383:999-1008
[4]. Hajar R 2017 Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views. 18(3):109-114
[5]. Ulbricht TL and Southgate DA 1991 Coronary heart disease: seven dietary factors. Lancet. 338(8773):985-92
[6]. Maas AH and Appelman YE 2010 Gender differences in coronary heart disease. Neth Heart J. 18(12):598-602
[7]. Murabito JM 1995 Women and cardiovascular disease: contributions from the Framingham Heart Study. J Am Med Womens Assoc1972). 50(2):35-9
[8]. Khayyam-Nekouei Z, Neshatdoost H, Yousefy A, Sadeghi M, and Manshaee G 2013 Psychological factors and coronary heart disease. ARYA Atheroscler. 9(1):102-111
[9]. Pathak LA, Shirodkar S, Ruparelia R, and Rajebahadur J 2017 Coronary artery disease in women. Indian Heart J. 69(4):532-538
[10]. Kuller LH 2010 Cardiovascular disease is preventable among women. Expert Rev Cardiovasc Ther. 8(2):175-87
[11]. Saeed A, Kampangkaew J, and Nambi V 2017 Prevention of Cardiovascular Disease in Women. Methodist Debakey Cardiovasc J. 13(4):185-192
[12]. Mann GV, Garrett HL, Farhi A, Murray H, and Billings FT 1969 Exercise to prevent coronary heart disease. An experimental study of the effects of training on risk factors for coronary disease in men. Am J Med. 46(1):12-27
[13]. Andersson C, Johnson AD, Benjamin EJ, Levy D, and Vasan RS 2019 70-year legacy of the Framingham Heart Study. Nat Rev Cardiol. 16(11):687-698
[14]. Andersson C, Nayor M, Tsao CW, Levy D, and Vasan RS 2021 Framingham Heart Study. JACC Focus Seminar, 1/8. J Am Coll Cardiol. 77(21):2680-2692
[15]. Tsao CW, and Vasan RS 2015 Cohort Profile: The Framingham Heart Study (FHS): overview of milestones in cardiovascular epidemiology. Int J Epidemiol. 44(6):1800-13
Cite this article
Shen,I. (2024). Cause disparities in coronary heart disease between genders. Theoretical and Natural Science,62,33-39.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Biological Engineering and Medical Science
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Sanchis-Gomar F, Perez-Quilis C, Leischik R, and Lucia A 2016 Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 4(13):256.
[2]. Kannel WB 1990 Bishop lecture. Contribution of the Framingham Study to preventive cardiology. 15(1):206-11
[3]. Mahmood SS, Levy D, Vasan RS, and Wang TJ 2014 The Framingham Heart Study and the Epidemiology of Cardiovascular Diseases: A Historical Perspective. Lancet. 383:999-1008
[4]. Hajar R 2017 Risk Factors for Coronary Artery Disease: Historical Perspectives. Heart Views. 18(3):109-114
[5]. Ulbricht TL and Southgate DA 1991 Coronary heart disease: seven dietary factors. Lancet. 338(8773):985-92
[6]. Maas AH and Appelman YE 2010 Gender differences in coronary heart disease. Neth Heart J. 18(12):598-602
[7]. Murabito JM 1995 Women and cardiovascular disease: contributions from the Framingham Heart Study. J Am Med Womens Assoc1972). 50(2):35-9
[8]. Khayyam-Nekouei Z, Neshatdoost H, Yousefy A, Sadeghi M, and Manshaee G 2013 Psychological factors and coronary heart disease. ARYA Atheroscler. 9(1):102-111
[9]. Pathak LA, Shirodkar S, Ruparelia R, and Rajebahadur J 2017 Coronary artery disease in women. Indian Heart J. 69(4):532-538
[10]. Kuller LH 2010 Cardiovascular disease is preventable among women. Expert Rev Cardiovasc Ther. 8(2):175-87
[11]. Saeed A, Kampangkaew J, and Nambi V 2017 Prevention of Cardiovascular Disease in Women. Methodist Debakey Cardiovasc J. 13(4):185-192
[12]. Mann GV, Garrett HL, Farhi A, Murray H, and Billings FT 1969 Exercise to prevent coronary heart disease. An experimental study of the effects of training on risk factors for coronary disease in men. Am J Med. 46(1):12-27
[13]. Andersson C, Johnson AD, Benjamin EJ, Levy D, and Vasan RS 2019 70-year legacy of the Framingham Heart Study. Nat Rev Cardiol. 16(11):687-698
[14]. Andersson C, Nayor M, Tsao CW, Levy D, and Vasan RS 2021 Framingham Heart Study. JACC Focus Seminar, 1/8. J Am Coll Cardiol. 77(21):2680-2692
[15]. Tsao CW, and Vasan RS 2015 Cohort Profile: The Framingham Heart Study (FHS): overview of milestones in cardiovascular epidemiology. Int J Epidemiol. 44(6):1800-13