






1. Introduction
As a common chronic disease, hypertension is the main risk factor for cardiovascular and cerebrovascular diseases. The diseases induced by it have extremely high mortality and disability rates, which not only greatly affect the normal behavior and life of residents, but also seriously consume medical and social resources [1]. Hypertension is divided into primary hypertension and secondary hypertension. The cause of the former is still unknown. But it is related to factors such as smoking, drinking, genetics, etc. The latter refers to an increase in blood pressure due to certain specific diseases or causes [2]. Therefore, this study is aimed at investigating secondary hypertension.
ACE is a key protein that induces hypertension and other related diseases, while ACEIs are important drugs for the treatment of hypertension and other diseases. Since the beginning of research on ACE inhibitors, there have been stable and mature drugs for the treatment of hypertension. ACE has two main functions. One is to catalyze the conversion of inactive angiotensin I into active angiotensin II, thereby increasing blood pressure. The second is to inactivate bradykinin and constrict blood vessels [3]. Because of these two functions, ACE has become an ideal target for the treatment of diseases such as hypertension, heart failure, type 2 diabetes, and diabetic nephropathy. The drugs developed for this target protein are Puli class drugs, such as Captopril, which is used to treat hypertension and heart failure; Enalapril maleate, which is used to treat essential hypertension and heart failure; Benazepril hydrochloride, which is used to treat various stages of hypertension and congestive heart failure [4]. At present, the specific pathogenesis of essential hypertension is still unclear, but there is a basic understanding of the pathogenesis of secondary hypertension. With further research, it has been found that the main pathogenesis of secondary hypertension revolves around the renin-angiotensin-aldosterone system (RAAS), and ACE inhibitors are important drugs that can affect its function [5].
This paper aims to investigate the structure and function of ACE, understand its functional structure, explore drugs targeting ACE for the treatment of hypertension, and provide reference and suggestions for future research on ACE and ACE inhibitors.
2. Functions and structure of ACE
2.1. Functions of ACE
There are many reasons that can cause blood pressure in the human body, such as abnormal sodium transport, sympathetic nervous system, renin-angiotensin system and bradykinin system, the lack of vasodilators. However, with further research, it has been found that the main reason for hypertension is caused by two mutually antagonistic systems, the renin-angiotensin system (RAS) and the kallikrein-kinin system (KKS). The main reason is the imbalance in regulation between the RSA and KKS systems, and angiotsin-converting enzyme plays a key role in the regulation of the two systems [5]. As shown in Figure 1, ACE converts inactive angiotensin 1 (Ang1) to active Ang2, which binds to its corresponding receptor and promotes vasoconstriction and the release of aldosterone to raise blood pressure [6]. On the other hand, bradykinin has the strongest effect on vasodilation, and ACE reacts enzymatically with bradykinin, causing it to lose its hypotensive function, resulting in an increase in blood pressure. Therefore, high levels of ACE in the body can cause the RSA and KKS systems to be out of balance, leading to an increase in blood pressure and worsening of related diseases [7]. In short, it can be used to lower blood pressure by inhibiting the activity of ACE in the body. It is important to study the catalytic mechanism of ACE and the inhibitory effect of inhibition of ACE.
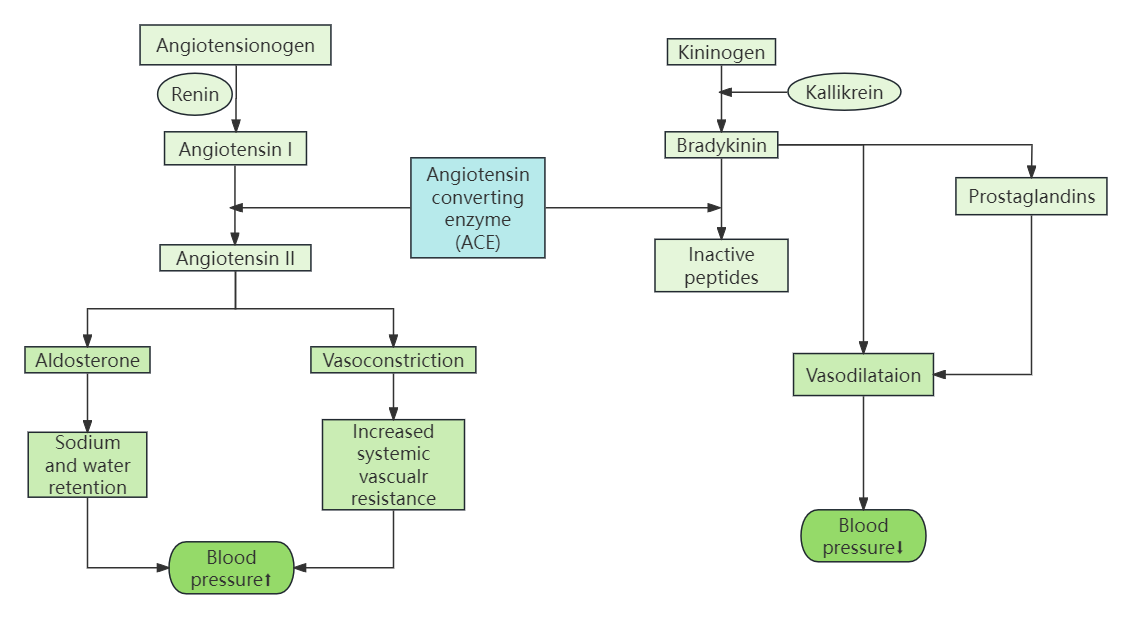
Figure 1. ACE action flow chart.
2.2. Functions of ACE inhibitors
By competitively inhibiting the converting enzyme, ACEI prevents angiotension I from being converted into angiotension II (AT II), which has the effect of vasoconstriction, resulting in vasodilation and decreased blood pressure. ACEI can inhibit the degradation of bradykinin, which can promote the production of vasodilator nitric oxide (NO) and prostatin by vascular endothelial cells, which directly exert vasodilator. For hypertensive patients with heart failure or diabetic nephropathy, ACE inhibitors are the drug of choice.
ACE inhibitors play an important role, which is manifested in the following aspects: (1) It can effectively combine with ACE, inhibit its flexibility, and reduce the content of angiotensin II, which can effectively reduce vascular volume and vascular resistance, and achieve the purpose of lowering blood pressure. (2) It can effectively regulate neuroendocrine, inhibit the release of catecholamines and aldosterone, improve the relaxation tension of blood vessels, and reduce the burden on the heart. (3) It can effectively inhibit the release of peptidase II, reduce the degradation rate of mitigation peptides, thereby stimulating the growth of β2 receptors to achieve the purpose of inhibiting platelet aggregation and effectively dilating blood vessels [8].
In addition to the above three effects, ACE inhibitors can also work together with angiotensin to lower blood pressure. The pharmacological analysis of ACE inhibitors: (1) can not only reduce blood pressure, but also ensure heart rate and cardiac excretion rate, inhibit the release of aldosterols and reduce the occurrence of sodium and water retention. At the same time, ACE inhibitors also have the effect of promoting deep circulation and helping to excrete sodium and water. (2) can effectively protect the target organs, promote the synthesis of collagen in the blood vessel wall and myocardial interstitium, prevent the occurrence of thickening of the blood vessel wall and myocardium, and reduce the burden on the heart, so it can effectively inhibit ventricular remodeling [9].
2.3. Designed with ACE as the target
With the development of science and technology, computer-aided drug design has become one of the important means of pharmaceutical research. The optimization of the model makes it increasingly feasible to simulate the interaction between drug and target protein molecule by computing. At present, molecular docking methods have become a common method to study the interaction patterns between small molecules and macromolecules, the recognition between biological macromolecules, molecular self-assembly, and supramolecular structure and so on.
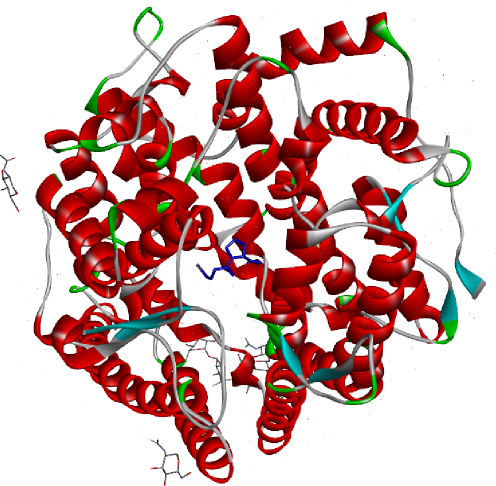
Figure 2. Receptor-ligand complex structure download from PDB database.
Captopril is the first orally synthesized non-peptide ACE inhibitor, which mainly acts on the renin-angiotensin-aldosterone system; Written descriptions do not provide a clear picture of the mode of action between captopril and ACE. A high-resolution crystal structure of the captopril with Drosophila ACE complex has been obtained (PDB: 2X8Z). In order to solve the above problems, the molecular docking function of DS molecular simulation software was used to design the docking experiment between captopril and ACE. Based on the PDB database, the receptor-ligand complex structure was obtained (Figure 2).
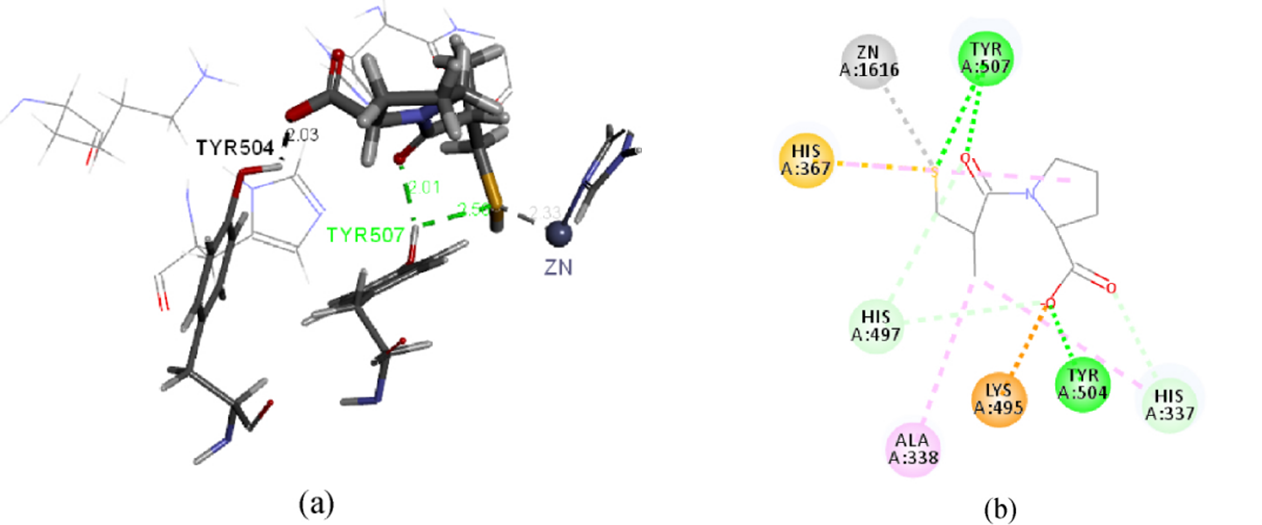
Figure 3. Diagram of interaction between captopril and ACE. (a: 3D diagram; b:2D diagram)
The interaction between captopril and ACE can be clearly seen in Figure 3. ACE is Zn-containing enzyme; Zn forms a stable coordination bond with the nitrogen atom of the amino acid residue HIS367 and is the active center of ACE. Zn plays an important role in the combination of captopril and ACE; S in captopril forms a coordination bond with Zn (bond length of 2.33 nm), which is an important binding site. The carbonyl and carboxyl groups of the captopril molecule form two other important hydrogen bonds with the acceptor. The carboxyl group and hydroxyl group on amino acid residue TRY504 form strong intermolecular hydrogen bonds with a bond length of 2.03nm. The carbonyl group and hydroxyl group on amino acid residue TRY507 form strong intermolecular hydrogen bonds with a bond length of 2.01nm. In addition to the coordination with Zn, S also has weak intermolecular hydrogen bond with the hydroxyl group on the amino acid residue TRY507, with the bond length of 2.56 nm. These sites of action are factors that need to be considered in the study of molecular structure-activity relationship and molecular structure modification.
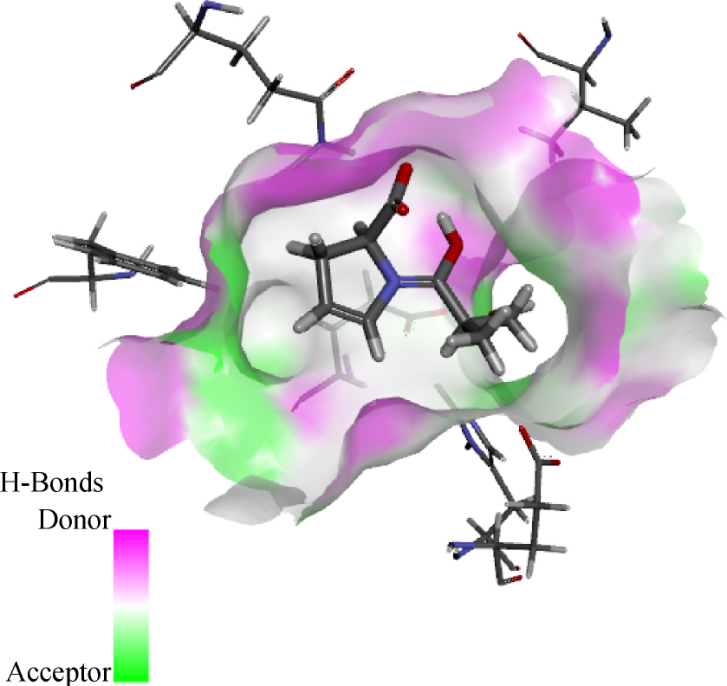
Figure 4. The H-Bonds surfaces on active site of ACE
The surface of the receptor’s H-Bonds is shown in Figure 4. Captopril molecule thiol groups penetrate deep into the cavity and bind with Zn ions. There is also a large cavity on the pyrrole ring side of L-proline; In the process of designing a new drug molecule, molecular fragments can be added to the cavity based on the hydrogen bond acceptor donor situation [10]. For example, a five-membered sulfur-containing heterocycle is attached to the pyrrole ring part of the spiropril molecule, which increases the molecular activity, which may be related to this spatial structure.
Captopril binds to ACE of Drosophila to form S-Zn coordination bond and three hydrogen bonds. These action sites are the factors to be considered in the study of molecular structure-activity relationship and molecular structure modification. Therefore, by changing the structure of small molecules, inhibitors that can act with ACE can be effectively designed
3. Drug targeting ACE-Benazepril
3.1. Benazepril
Benazepril is a kind of nonsulfhydryl ACE inhibitor that has good pharmacodynamic and pharmacokinetic properties as well as efficientantihypertnsive effects and a excellent tolerability. As a prodrug, Benazepril can be hydrolyzed into the active substance called Benazeprilat, as shown in Figure 5. Both Benazepril and Benazeprilat has ability to inhibit the normal function of ACE and the inhibition effect of Benazeprilat is much better than that of Benazepril. The chemical name is 3-([1-ethoxycarbonyl-3-phenyl-(1S)-propyl]-amino)-2,3,4,5tetrahydro-2-oxo-1(3S)-benzazepine-1-acetic acid.
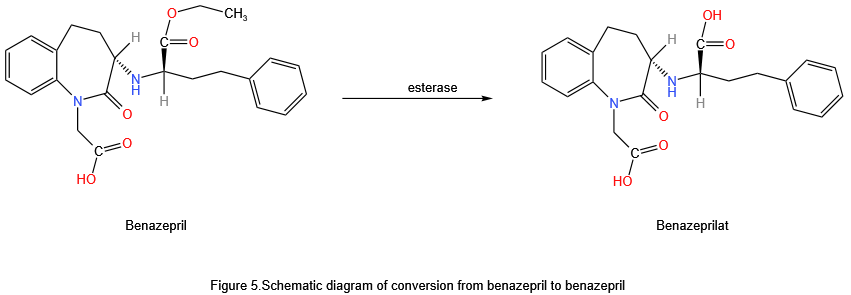
Figure 5. Schematic diagram of conversion from benazepril to benazeprilat.
3.2. Availability of benazepril in the treatment of patients with renal insufficiency
Renal dysfunction caused by many complicated factors, is a state that the body become hard to excrete metabolites and keep the regulation of water, electrolytes and acid-base balance, including acute renal insufficiency and chronic renal insufficiency. The hypertensive patients with well-being renal function excrete medicines by kidneys, while the patients with renal insufficiency are unable to excrete drugs as normal. Because Benazepril can be excreted via both kidneys and bile [10], when the kidneys have trouble eliminating the drug, bile is qualified to replace kidneys to excrete the metabolites of the Benazepril, avoiding the adverse reaction induced by excessive remaining drugs and metabolites in the body. Wang, et al. did research on the influence of Benazepril on proteinuria and renal function in patients with renal hypertension, dividing a totally of 53 patients with renal hypertension into the group with normal renal function and the group with renal insufficiency according to the distinct level of blood urea nitrogen and blood creatinine. Benazepril was provided to patients whose systolic blood pressure ≥ 18.7kPa and diastolic blood pressure ≥ 12kPa, beginning with a few doses and controlling the usage of the dose according to the daily blood pressure level [11]. This cure process continued for 4 weeks in both groups. Blood pressure was measured every day and the final value of blood pressure at week 4 was used as the standard. Venous blood was drawn on an empty stomach to measure blood glucose, blood creatinine, and urea nitrogen before the dose and at the end of the 4th week, and 24-hour urine protein quantification and routine electrocardiograms were measured. This study had found that Benazepril had an obvious effect on treating the renal hypertension, which proved that the the better therapeutic effect of Benazepril in hypertensive patients with renal insufficiency.
3.3. The mechanism of benazepril on hypertension
At the first, Benazepril yields Benazeprilat via hydrolysis in the body by the enzymes. Then, both Benazepril and Benazeprilat competes with the ACE for binding the reception, thereby reducing the ACE activity, blocking the course that ACE turns angiotnsin I into angiotensin II, so that angiotensin receptor can not be motivated and the release of the aldosterone will decrease, thus the whole body of the peripheral vasculature diastolic, reduce vascular resistance. As a result, the blood pressure declined.
3.4. Adverse reactions and matters need attention of the benazepril
The side effects probably caused by the usage of Benazepril are separated into slight and severe adverse reactions depending on the diverse extent of the onset. Slight adverse reactions mainly include cough, first dose hypertension and hyperkalemia. Severe adverse reactions largely contain pregnancy risk and angioneurotic edema, etc. [12] Now, irritating dry cough is an adverse reaction with a higher incidence, characterized by cough and pharyngeal discomfort, which disappears after a week of withdrawal of the drug at a large margin. Due to the tolerance in most cases, patients would not need to withdraw the drug. For patients who have first dose hypertension, the medicine should be started at a small dose and concomitant use with diuretics should be avoided. For hyperkalemia caused by Benazepril, patients should be started at a few dose of the drug and progressively rose to the target dose and blood potassium concentration should be detected regularly. If there are evident lethargy, drowsiness, muscle weakness, cold hands and feet, and sluggishness during the therapy, the drug must be stopped immediately. Angioneurotic edema [13] is actually a more dangerous symptom comparing to other side effects so that medications should be discontinued immediately and airway function must be kept properly when it occurs. Epinephrine should be injected subcutaneously when the airway has some problems, and saline should be given intravenously if hypotension appears. Add to that, the medicines belonging to ACEI are prohibited for utilize to women that are pregnant.
4. Conclusion
Due to the increasing attention to hypertension, the role of the renin-angiotensin-aldosterone system in hypertension has been studied more and more clearly. In this paper, through the study of the structure and function of ACE, we discussed the design method of ACEI as the target drug, and pointed out that it is very convenient and efficient to design drugs with ACE as the target, and then we envisioned that computer simulation of molecular docking technology can be combined with the design of drugs with biomolecules as the target, and we can understand the docking of small molecules and biomolecules clearly through this convenient method, and thus modify the parent drug to design drugs for different patients. This is a convenient way to clearly understand the docking of small molecules with biomolecules, which can be used to modify the parent drug to design drugs for different patients. We also discussed the application of Benazepril in hypertension. Since the introduction of captopril, there have been many Prilosec drugs targeting ACE, and by exploring the combination of ACE and ACEI and Benazepril, we hope to provide more methods and ideas for drug design by target.
Authors Contribution
All the authors contributed equally and their names were listed in alphabetical order.
References
[1]. Wang J F Zhou W Zhao S et al 2022 Analysis of the effects of angiotensin-converting enzyme inhibitor drugs in the treatment of hypertension Medical Diet and Health 20 16 44-46
[2]. Zhu J Q & Tuo X P 2022 Current status of diagnosis and treatment of secondary hypertension Chinese Journal of Clinical Health 25 05 610-613
[3]. Hu Y Qiu C C & Li J P 2018 Research progress on the relationship between angiotensin-converting enzyme and hypertension Journal of Medical Research 47 11 15-18
[4]. Li G W Dai H B & Shi J N 2023 Angiotensin-converting enzyme inhibitors: A series of guides for antihypertensive drug use I China Rational Drug Use Exploration 20 04 1-6
[5]. Qin M Y Yang W Lü Y Y et al 2022 Research progress on multi-target intervention treatment of hypertension with renin-angiotensin-aldosterone system inhibitors Modern Drugs and Clinical 37 02 439-444
[6]. Ma H Y Wang N & Yang L X 2023 Research progress on aldosterone levels and cardiovascular diseases China Medical Innovation 20 22 176-180
[7]. Xiong Z A 2018 Research on the extraction of angiotensin-converting enzyme and its interaction with inhibitors [Master's thesis Guangxi University]
[8]. Xiao Z H nd Analysis of angiotensin-converting enzyme inhibitor treatment for hypertension PDF Document
[9]. Xu B 2018 Mechanism of cardiovascular protective effects of angiotensin-converting enzyme inhibitors Chinese Journal of Hypertension 26 09 813-816
[10]. Huang X R 1999 The efficacy of benazepril in the treatment of hypertension and its effects on liver and kidney function blood lipids and blood glucose Chinese Journal of Modern Medicine 08 21-22
[11]. Wang L X Wu C S & Liang H X 2000 The effects of benazepril on renal hypertension proteinuria and renal function Zhongyuan Medical Journal 08 17-18
[12]. Ren X L Yang L & Li Y Z 2010 Analysis of adverse reactions caused by ACEI drugs and clinical rational drug use Chinese Hospital Drug Evaluation and Analysis 10 09 837-839
[13]. Vleeming W van Amsterdam J G Stricker B H & de Wildt D J 1998 ACE inhibitor-induced angioedema: Incidence prevention and management Drug Safety 18 3 171-188
Cite this article
Li,S.;Zhu,M. (2024). Functional structure of angiotensin-converting enzyme (ACE) and its targeted drugs. Theoretical and Natural Science,62,88-94.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Biological Engineering and Medical Science
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Wang J F Zhou W Zhao S et al 2022 Analysis of the effects of angiotensin-converting enzyme inhibitor drugs in the treatment of hypertension Medical Diet and Health 20 16 44-46
[2]. Zhu J Q & Tuo X P 2022 Current status of diagnosis and treatment of secondary hypertension Chinese Journal of Clinical Health 25 05 610-613
[3]. Hu Y Qiu C C & Li J P 2018 Research progress on the relationship between angiotensin-converting enzyme and hypertension Journal of Medical Research 47 11 15-18
[4]. Li G W Dai H B & Shi J N 2023 Angiotensin-converting enzyme inhibitors: A series of guides for antihypertensive drug use I China Rational Drug Use Exploration 20 04 1-6
[5]. Qin M Y Yang W Lü Y Y et al 2022 Research progress on multi-target intervention treatment of hypertension with renin-angiotensin-aldosterone system inhibitors Modern Drugs and Clinical 37 02 439-444
[6]. Ma H Y Wang N & Yang L X 2023 Research progress on aldosterone levels and cardiovascular diseases China Medical Innovation 20 22 176-180
[7]. Xiong Z A 2018 Research on the extraction of angiotensin-converting enzyme and its interaction with inhibitors [Master's thesis Guangxi University]
[8]. Xiao Z H nd Analysis of angiotensin-converting enzyme inhibitor treatment for hypertension PDF Document
[9]. Xu B 2018 Mechanism of cardiovascular protective effects of angiotensin-converting enzyme inhibitors Chinese Journal of Hypertension 26 09 813-816
[10]. Huang X R 1999 The efficacy of benazepril in the treatment of hypertension and its effects on liver and kidney function blood lipids and blood glucose Chinese Journal of Modern Medicine 08 21-22
[11]. Wang L X Wu C S & Liang H X 2000 The effects of benazepril on renal hypertension proteinuria and renal function Zhongyuan Medical Journal 08 17-18
[12]. Ren X L Yang L & Li Y Z 2010 Analysis of adverse reactions caused by ACEI drugs and clinical rational drug use Chinese Hospital Drug Evaluation and Analysis 10 09 837-839
[13]. Vleeming W van Amsterdam J G Stricker B H & de Wildt D J 1998 ACE inhibitor-induced angioedema: Incidence prevention and management Drug Safety 18 3 171-188