






1. Introduction
Both professional and recreational sports are seeing an increase in hamstring injuries, necessitating a specific focus on prevention and rehabilitation. The "hamstrings" consist of the thigh's posterior muscles: semitendinosus (ST), biceps femoris (BF), semimembranosus (SM), short head (BFSH) and long head (BFLH). The muscle group of the long hamstrings (ST, BF, SM, BFSH, BFLH) traverses both the hip joints and knee joints, hence it plays a part in hip extension, knee flexion, and internal (SM and ST) or external knee rotation (BF), during concentric contraction [1]. When there is a muscular imbalance, while the hamstrings are not adequately warmed up or are fatigued, or when there is any sudden need for speed will cause hamstring injuries and this particular muscle group will experience a high frequency of injuries. Besides, hamstring injuries are common among athletes, particularly, athletes who play sports like basketball, track, or soccer that demand sprinting. This article will focus on the causes of the disease by analyzing the mainly injured part of hamstring injuries and anatomy of people’s bone structure. Given how common hamstring injuries are among football players, and the re-injured rate is still increasing in recent years, analysis among the population that will develop this disease, and the severity of the disease based on the mechanisms of the injury would also report. Also, some corresponding effective treatments and prevention of each different kinds of hamstring injury are presented. This article will provide a comprehensive analysis of the hamstring injuries from both past and recent information.
2. Anatomy
The main structures in which hamstring injuries happen are the proximal insertion, Proximal Tendons and Musculotendinous Junctions, Distal Tendons and Musculotendinous Junctions, and Distal insertion.
2.1. Proximal insertion
The proximal insertion of the Semimembranosus (SM) is typically characterized as the lateral surface of the ischial tuberosity. This insertion is positioned laterally and anteriorly relative to the start of the conjoined tendon formed by the Biceps Femoris Long Head (BFLH) and Semitendinosus (ST), while being located posteriorly (superficially) to the quadratus femoris muscle's origin. A type of "conjoined tendons" made up of the BFLH and ST tendons emerges from the posteromedial portion of the ischial tuberosity [2]. The robust, rounded tendon of the BFLH occupies the lateral region of the medial facet and has attachments to the sacrotuberous ligament. The Biceps Femoris Short Head (BFSH) begins about 15 cm below the distal insertion point of the gluteus maximus (GM), starting just distal to the ischial tuberosity.
2.2. Proximal tendons and musculotendinous junctions
The musculotendinous junction (MTJ), where the muscle fibers attach to the tendon, and the "free" tendons, that has no muscular fascicle changes, make up the tendons of the hamstring muscles [3].
The tendon of Semimembranosus, originating from the ischial tuberosity, is inserted from the posterior upper end of the tibia and is mostly used for thigh extension, calf flexion, and a minor inward rotation. It comes from the musculotendinous connections and proximal tendons. The proximal SM ligament is an essential component of the posteromedial quadrant on the knee, together with the anterior obtuse ligaments, posterior horn of the medial meniscus, and medial collateral ligament. At knee joints, SM probably serves as an active constraint against external rotation (with knee flexion) and valgus (when the knee is stretched). Among all the hamstring muscles, the SM proximal tendon is the longest, measuring around 32 cm which makes up approximately 75% in the whole muscle length.
2.3. Distal tendons and musculotendinous junctions
The medial facet or posteromedial region of the ischial tuberosity is where the semitendinosus muscle begins, and it attaches to the medial part of the tibia. It encourages internal rotation, leg flexion, and thigh extension at the hip joint.
The BFsh (Biceps Femoris Short Head) starts near the lateral femur and intermuscular septum, with a portion of the tendinous tissue, about connecting the muscle to the bone. Whereas every tissue are not exists intramuscularly in the proximal area of the muscle. The MTJ, which is situated along the aponeurosis on the front of the muscle and the linked tendon, is therefore negligible since BFSH fascicles emerge directly from their proximal insertion sites into this small quantity of tendinous tissue [3].
2.4. Distal insertion
Biceps femoris long and short which is individually from the ischial tuberosity and the crista femoris, are inserted until the fibular head, and their primary roles include flexing and medially rotating legs and extending the lower leg at the hip joint.
3. Mechanism
The two primary mechanisms of hamstring injuries are stretch and sprint.
3.1. The stretch
This kind of mechanism really commonly occurs due to extensive hip flexion with a hyperextended knee, which places a large strain on the hamstring muscles, such as the kicking or the splits in dance. Apart from that, this mechanism always affects the semimembranosus muscle. For instance, during the stance phase, when the feet are contact with the ground, the body will experience forces as it propels forward over the foot. Some studies suggested that hamstring injuries might occur during the early stance phase due to large opposing forces as the body moves forward over the touchdown point.
3.2. The sprint
This type of mechanism often impacts the lengthy head of the biceps femoris muscle and happens in the final swing stage of the running gait cycle, while the hamstring muscles are stretching under eccentric contraction right prior to the foot strike. During the swing phase when the foot is off the ground, it is divided into different sub-phases, with the late or terminal swing phase being particularly important. During the late swing phase, the hamstring muscles lengthen under load in an eccentric contraction as the leg prepares for the foot strike.
4. Risk factors
4.1. Non-modifiable risk factors
The age is important to take an account in older athletes who have an increased risk of hamstring strains and also decreased flexibility and muscle elasticity. Besides, people who already have similar injuries before would also significantly increase the risk of injured again, with re-injured rates being notably high in the first week of getting back into sports.
4.2. Modifiable risk factors
Apart from the previous factors, is the modifiable risk factors. People with muscle weakness and fatigue are more susceptible to injury, especially when exposed to high-speed running or sudden changes in direction and is better for those people to take the time to do the recovery. Lower levels of eccentric knee flexor strength significantly elevated the risk rate of future hamstring injuries, according to research on knee flexor strength that involved 190 patients with hamstring strains among 614 elite Qatari football players (OR=1.37; 95% CI=1.01–1.85) [3]. If people have less muscle balance, it is possible to get hamstring injuries. Similar to muscle imbalances, A growing risk of injury is closely linked to a strength imbalance between the eccentric and concentric strength of the hamstrings and quadriceps. Higher levels of strength seemed to offset the risk of injury associated with getting older or having a history of hamstring injury in the studies that found a correlation between eccentric strength and injury rates. These interactions also emerged between eccentric strength, age, and prior hamstring injury [4]. Also, limited hamstring flexibility can contribute to the likelihood of injury, as can tightness in the quadriceps and hip flexes. Poor Neuromuscular Control, which means the inadequate coordination and control of the muscles around the pelvis and truck can lead to inefficient movement patterns and increase risks.
5. Treatment
5.1. Non-operative management techniques
When treating acute hamstring injuries, nonoperative management techniques play a crucial role. The POLICE principle—Protection, Optimal Loading, Ice, Compression, and Elevation—is widely recognized for managing soft tissue injuries.
Protection: This involves safeguarding the injured area to prevent further damage. By avoiding activities that stress the injury which can minimize additional harm.
Optimal Loading: Instead of complete rest, balanced and incremental loading is recommended. This approach allows for a gradual increase in activity, promoting healing while reducing the danger of getting hurt again.
Ice: Applying ice on injured area 2 to 3 times per day can significantly reduce pain and inflammation. It’s an effective method for managing the initial swelling and discomfort.
Compression: Using a simple malleable bandage or an inflatable cylindrical bandage from a pharmacy or clinic, people can compress or bind their thighs to minimize swelling and movement that might result in additional damage.
Elevations: To lessen any swelling, patient should try to keep their legs up and hold by a cushion as much as possible.
Through those kinds of treatments, the acute soft tissue injuries will be significantly reduced. Athletes who do have less severe injuries can return to sports immediately, others who have more serious injuries will have less pain and reduce the inflammation, then can continue the next section of the rehabilitation program.
For managing pain and inflammation, NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) are often used, which has less risks and can spend less costs. These medications can reduce pain and allow for increased activity during physical therapy. However, they may also impact muscle function during recovery. The effects of NSAIDs on proximal hamstring injuries are not fully understood, so their use should be discussed with a healthcare provider to weigh the benefits and risks.
5.2. Physiotherapy
Once inflammation and pain are under control, physiotherapy becomes a key component of recovery. Effective physiotherapy treatments include both eccentric strength training and trunk stabilization [5].
First of all, the eccentric strength training involves exercises (Nordic Hamstring Curls, The Extender, The Driver) which designed to increase hamstring flexibility and strength. Combined the exercise for strength and pelvis stabilization, which also give more specific strength training exercise. Besides, it contains 3 steps of exercises, the first one is the Nordic Hamstring Curls (By placing the athlete’s knees on a surface while another people need to catch their heels), then the Extender (With the injured hip and knee flexed to 90°, then required athletes slowly extend their knee.). Finally, is the Driver (Lean forward to a 90° hip flexion while standing on the injured leg and extending the athlete's arms forward).
Another effective physiotherapy treatment is called trunk stabilization (Side bridges (Planks), Single-leg standing windmill, Lunge twist), which can help athletes to Improve their pelvic positioning, in order to facilitate optimal tendon tension [6]. This rehabilitation program also contains three steps of exercise, the first one is side bridges or called Planks ( Requiring athletes to support their body by placing the ankle and elbow in one side.), then athletes are required to do the Single-leg standing windmill (Standing by the injured hip, then lean forward ), the last action required is Lunge twist (Standing in the standard lunge position, turn torso toward the bent knee).
Through those two kinds of rehabilitation program, athletes can recover better, which can help them to improve the hamstring flexibility.
There are also have a study of the comparison about the mainly eccentric exercises program (L-protocol group, mainly focus on the muscle flexibility training) and the less emphasis eccentric exercises program (C-protocol group, less focus on the eccentric training instead of muscle strength training). The study involves the team of male soccer athletes, and by organizing them into two groups. One is the controlled group who is trained in the mainly eccentric exercise (L-protocol group) and the other one is less focus on the eccentric training (C-protocol group) [7]. Research shows that the L-protocol exercise strength program is more effectively than the C-protocol exercise and any other traditional resistance training exercises, which result in better adaptions of the position of peak toque, concentric hamstring to quadriceps strength ratio and vertical jump performance. Also increase hamstring flexibility. Reduce the risk of the recur. This kind of rehabilitation is useful for every athlete, especially for the athletes who has prior hamstring injuries. In short, a program for rehabilitation that mostly consists of eccentric exercises is more reliable and efficient, lowering the rates of hamstring re-injury and assisting in the restoration of the ideal muscular tendon length for tension generation (as shown in Figure 1and 2) [8].
Apart from that, some new neural mobilization techniques are also useful for athletes during the rehabilitation. This technique includes two different types. One is the neural slider; during the first stage, participants were placed high on a plinth to make sure their feet cannot contact the ground, and their hands should be placed on their backs. Then, while maintaining ankle dorsiflexion, stretch the cervical area and the knee. During the second stage. Participants were instructed to simultaneously do the ankle extension, flex the knee and the cervical region. Each set contain 30 repetitions, each of which had to be completed in 2 seconds, contain a 30 second break interval between training. The other technique is termed neural tension; in the first step, participants must flex the neck region also extending the knee and dorsiflexing the ankle. During the next stage, participants were instructed to keep the ankle dorsiflexion and cervical flexion, then flex the knee simultaneously. Similarly to the previous technique, one set consisted of 30 repetitions, and each set had to be done in 2s, for a total of 30 repeating workouts in the 60s. For every extremity, three sets were done in turn. The sets were separated by a 30-second rest time. The organization of the two techniques is similar [9].
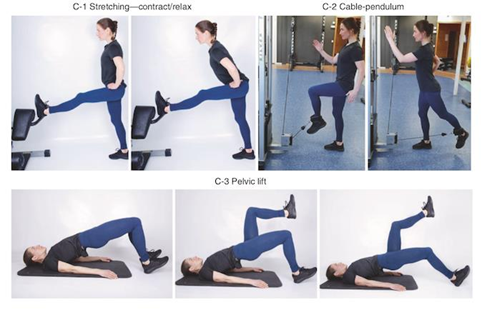

Figure 1: C-protocol (left) [8]. Figure 2: L-protocol (right) [8]
6. Prevention
6.1. Warm-up
Since improper warm-up techniques may raise the risk of subsequent hamstring injuries, an appropriate warm-up is thought to be essential for overall injury avoidance. Some beneficial and effective warm-up regimens include Nordic, Russian, and Hamstring Lowers. Furthermore, FIFA 11, a pre-training warm-up designed specifically to avoid lower limb injuries in soccer, serves as one of the most popular and frequently utilized preventative regimens [10].
6.2. Eccentric strength training
Injury to the hamstrings is possible, especially when exercising with a component of eccentric stress. which minimizes the dangers of hamstring injury as long as the intervention is followed properly. Despite a full RTS, athletes may experience eccentric weakness and reduced torque development 1-36 months post-injury [11]. Peak eccentric knee flexor effort and power deficits were around 10% and 13%, respectively, for athletes who had second-degree or third-degree injuries 19 ±12.5 months before isokinetic evaluation, according to Lee and colleagues. There have also been reports of deficiencies in the biceps femoris long head (BFLH) [12].
6.3. Stretching
The study about soccer players concluded that stretching was used as part of a preventative program. The team suffered eight hamstring injuries in the two years after the intervention's adoption, and 27 in the two years before. Furthermore, this led to a notable decrease in the number of games missed due to injuries [13].
7. Conclusion
Acute hamstring injury, hamstring damage with sequela (recurrent episodes of injury and/or pain), and hamstring tendinopathy are the three clinical scenarios into which hamstring injuries can be divided. By analyzing the anatomy of potential injured area, it can clearly show the composition of the injuries. Two mechanisms are present in the hamstring injuries, which is sprinting and stretch. The most well recognized factors that increase an athlete's risk of hamstring strains are increased age chronologically, a previous record about hamstring strains, and decreasing eccentric strength. Nevertheless, even among these often examined criteria, there is no total consensus in the results. Then during the rehabilitation, athletes should follow the order of recovery, from soft tissue injuries to inflammation and then focus on the muscle strength and flexibility training, which can help athletes to go back to sports more quickly. For managing simple or the surface of the injuries, traditional treatment such as POLICE principles is very useful and safety. There is mounting evidence that eccentric-biased training at progressively longer muscle lengths, early loading, and rehabilitation are all more crucial for treating acute hamstring muscular strain injuries. Apart from that, the innovative techniques such as neural slider and neural tension also play a big role during the recovery of athletes.
References
[1]. Verrall GM, Slavotinek JP, Barnes PG. The effect of sports specific training on reducing the incidence of hamstring injuries in professional Australian Rules football players. Br J Sports Med. 2005;39:363–8.
[2]. Chang, J. S., Kayani, B., Plastow, R., Singh, S., Magan, A., & Haddad, F. S. (2020). Management of hamstring injuries: Current concepts review. The Bone & Joint Journal, 102-B(10), 1281–1288. https://doi.org/10.1302/0301-620X.102B10.BJJ-2020-1210.R1
[3]. van Dyk N, Bahr R, Whiteley R, Tol JL, Kumar BD, Hamilton B, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44(7):1789–95.
[4]. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in australian footballers. Med Sci Sports Exerc. 2014;47(4):857–65.
[5]. Youm, T. (Ed.). (2021). Proximal Hamstring Tears: From Endoscopic Repair to Open Reconstruction. Springer International Publishing. https://doi.org/10.1007/978-3-030-56025-6 (zhiliao)
[6]. Heiderscheit, B. C., Sherry, M. A., Silder, A., Chumanov, E. S., & Thelen, D. G. (2010). Hamstring strain injuries: Recommendations for diagnosis, rehabilitation and injury prevention. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 67–81. https://doi.org/10.2519/jospt.2010.3047
[7]. Pas HIMFL, et al. Br J Sports Med 2015;Efficacy of rehabilitation (lengthening) exercises, platelet-rich plasma injections, and other conservative interventions in acute hamstring injuries: an updated systematic review and meta-analysis49:1197–1205. doi:10.1136/bjsports-2015-094879
[8]. Schroeter, S., Heiss, R., Hammer, C. M., Grim, C., Engelhardt, M., & Hotfiel, T. (2022). Diagnosis of Proximal Hamstring Injuries. Sports Orthopaedics and Traumatology, 38(1), 47–57. https://doi.org/10.1016/j.orthtr.2022.01.008
[9]. Schmitt B, Tim T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. Int J Sports Phys Ther. 2012;7(3):333.
[10]. Croisier JL, Forthomme B, Namurois MH, Vanderthommen M, Crielaard JM. Hamstring muscle strain recurrence and strength performance disorders. Am J Sports Med. 2002;30(2):199–203.
[11]. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. The effect of previous hamstring strain injuries on the change in eccentric hamstring strength during preseason training in elite Australian footballers. Am J Sports Med. 2015;43:377–84.
[12]. Thorborg, K., Opar, D., & Shield, A. (Eds.). (2020). Prevention and rehabilitation of hamstring injuries. Springer Nature Switzerland. https://doi.org/10.1007/978-3-030-31638-9
[13]. Chu, S. K., & Rho, M. E. (2016). Hamstring Injuries in the Athlete: Diagnosis, Treatment, and Return to Play. Current sports medicine reports, 15(3), 184–190. https://doi.org/10.1249/JSR.0000000000000264
Cite this article
Li,Y. (2025). Analysis of the Hamstring Injuries among Soccer Athletes. Theoretical and Natural Science,68,39-45.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 3rd International Conference on Modern Medicine and Global Health
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Verrall GM, Slavotinek JP, Barnes PG. The effect of sports specific training on reducing the incidence of hamstring injuries in professional Australian Rules football players. Br J Sports Med. 2005;39:363–8.
[2]. Chang, J. S., Kayani, B., Plastow, R., Singh, S., Magan, A., & Haddad, F. S. (2020). Management of hamstring injuries: Current concepts review. The Bone & Joint Journal, 102-B(10), 1281–1288. https://doi.org/10.1302/0301-620X.102B10.BJJ-2020-1210.R1
[3]. van Dyk N, Bahr R, Whiteley R, Tol JL, Kumar BD, Hamilton B, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44(7):1789–95.
[4]. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in australian footballers. Med Sci Sports Exerc. 2014;47(4):857–65.
[5]. Youm, T. (Ed.). (2021). Proximal Hamstring Tears: From Endoscopic Repair to Open Reconstruction. Springer International Publishing. https://doi.org/10.1007/978-3-030-56025-6 (zhiliao)
[6]. Heiderscheit, B. C., Sherry, M. A., Silder, A., Chumanov, E. S., & Thelen, D. G. (2010). Hamstring strain injuries: Recommendations for diagnosis, rehabilitation and injury prevention. Journal of Orthopaedic & Sports Physical Therapy, 40(2), 67–81. https://doi.org/10.2519/jospt.2010.3047
[7]. Pas HIMFL, et al. Br J Sports Med 2015;Efficacy of rehabilitation (lengthening) exercises, platelet-rich plasma injections, and other conservative interventions in acute hamstring injuries: an updated systematic review and meta-analysis49:1197–1205. doi:10.1136/bjsports-2015-094879
[8]. Schroeter, S., Heiss, R., Hammer, C. M., Grim, C., Engelhardt, M., & Hotfiel, T. (2022). Diagnosis of Proximal Hamstring Injuries. Sports Orthopaedics and Traumatology, 38(1), 47–57. https://doi.org/10.1016/j.orthtr.2022.01.008
[9]. Schmitt B, Tim T, McHugh M. Hamstring injury rehabilitation and prevention of reinjury using lengthened state eccentric training: a new concept. Int J Sports Phys Ther. 2012;7(3):333.
[10]. Croisier JL, Forthomme B, Namurois MH, Vanderthommen M, Crielaard JM. Hamstring muscle strain recurrence and strength performance disorders. Am J Sports Med. 2002;30(2):199–203.
[11]. Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. The effect of previous hamstring strain injuries on the change in eccentric hamstring strength during preseason training in elite Australian footballers. Am J Sports Med. 2015;43:377–84.
[12]. Thorborg, K., Opar, D., & Shield, A. (Eds.). (2020). Prevention and rehabilitation of hamstring injuries. Springer Nature Switzerland. https://doi.org/10.1007/978-3-030-31638-9
[13]. Chu, S. K., & Rho, M. E. (2016). Hamstring Injuries in the Athlete: Diagnosis, Treatment, and Return to Play. Current sports medicine reports, 15(3), 184–190. https://doi.org/10.1249/JSR.0000000000000264