






1. Introduction
Hypertension, commonly known as high blood pressure, impact on people’s health by its harmful symptoms, include heart stroke, blood vessel disease, and kidney damage [1]. According to the World Health Organization (WHO), approximately 1.28 billion people aging from 30-79 years suffered from hypertension [1]. Based on the widespread impact of hypertension on society, establishing effective methods to prevent and treat hypertension requires more attention [2-8]. Some studies pointed out that there is a relationship between hypertension and caffeine [2,3]. Many foods or beverages containing caffeine serve as natural stimulants to provoke the neuron system and accelerate the heart rate, systolic forces, and diastolic forces, which will affect blood pressure theoretically. Discover the correlation between caffeine intake and hypertension would help us understanding the undergo mechanism of hypertension and seek insights of benefits from caffeine.
Although a lot of research has been conducted to investigate the specific relationship between caffeine intake and hypertension, debates still exist in the field of science. Some research considered that coffee intake plays a small role in increasing and developing hypertension [3,9]. On the contrary, some scientists claimed that consuming an appropriate amount of caffeine will either protect the heart and blood vessels or irrelevant with hypertension [4-5]. In these literatures, authors claimed that with more caffeine intake will benefit the prevention of hypertension. Therefore, the relationship between caffeine intake the risk of hypertension remained controversy on whether it could benefit the prevention of hypertension and thus needed more attention. Furthermore, some studies suggested that the relationship between caffeine intake and the risk of hypertension was inverse U-shaped [2,6], which gave an insight that caffeine intake could have inverse relationship to risk of hypertension depending on the amount of consumption. Others instead stated that there was no or a little non-linear relationship between the caffeine intake and hypertension [10,11]. The research mentioned above produced many controversies and differences. However, we still lack a uniform consensus on the correlation between caffeine intake and hypertension.
While previous studies have provided valuable insights, significant limitations and research gaps still exist. Notably, many prospective observational studies have been constrained by their narrow population focus, hindering the generalizability of their findings across diverse demographic groups, including gender, age, and ethnicity [3,7]. Similarly, in some studies, BMI (body mass index) [10], smoking [6], alcohol consumption [6,10], sodium intake [10], and other factors [6,10] were not included in the analysis as covariates, further limiting the comprehensiveness and depth of these studies.
This study aims to fill current research gaps and address the shortcomings of existing research through a more comprehensive research design. The primary objective of this study is to delve into the specific association between caffeine intake and hypertension risk, through detailed data analysis and model construction, reveal the underlying correlations and assist with the public health policy formulation and individual health management.
2. Methodology
2.1. Study population
The research objects of this study are from the participants of National Health and Nutrition Examination Survey (NHANES). NHANES is designed to collect data on the diet, nutritional status, health, and health behaviors of non-institutionalized US populations. The data were collected through home interviews, followed by specific inspection and medical examination and interviews.
Dietary data were collected using a combination of 24-hour food recall and food frequency questionnaires. The dataset has been filtered and will be further screened to ensure a diverse and representative sample. Further screening would facilitate the analysis of the relationship between caffeine intake and the risk of high blood pressure.
2.2. Blood Pressure and Hypertension
The outcome variable of concern in this study was the presence of hypertension. Researchers measured blood pressure in participants aged 8 years and older. Three measurements were taken. The first read was to make good preparations. The second is to maintain the correct posture. The third is to operate the blood pressure monitor (repeat the measurement at least three times at 1–2-minute intervals). The last is to record and analyze. The purpose of the first blood pressure measurement is to obtain preliminary information about the participant's blood pressure at a given moment in time. However, pre-measurement activities and emotional state may affect the first measurement, resulting in some errors. The purpose of the second measurement is to reduce the chance of errors. The third measurement further validates the stability of the blood pressure and ensures accurate and consistent readings. In this study, a sample with diastolic blood pressure greater than 90 mmHg or systolic blood pressure greater than 140 mmHg is defined as hypertensive patients [1].
2.3. Caffeine Consumption
The main contributing factor in this study was caffeine intake. The data was collected in the mobile examination center (MEC) diet interview room. Participants would be provided with a set of measurement guidelines so that they could review what they eat. At the end of the interview, participants were given measuring cups, spoons, rulers, and a food modeling booklet, as well as 2D drawings containing guidelines for the various measurements available in the MEC. These tools were used to collect food types and quantities during telephone interviews.
2.4. Assessment of covariates
In addition to these two factors, several key covariates were considered to control for potential confounders. These include body mass index (BMI), smoking status, alcohol consumption and dietary salt intake. BMI could be calculated by measuring the height and weight of the participants. Data on smoking and alcohol use were obtained from home interview questionnaires. Dietary salt intake was estimated based on 24-hour dietary recall data. Standardized protocols were used in the process of collecting these variables, while other factors that could affect blood pressure were considered. This ensured a more comprehensive and accurate assessment of the relationship between caffeine intake and high blood pressure.
2.5. Statistical Analysis
Blood pressure was measured three times in the NHANES, and both diastolic and systolic blood pressure were measured each time. Therefore, the average of obtained blood pressure measurements was chosen as diastolic and systolic blood. Caffeine intake, alcohol intake, and sodium intake were averaged over two days (or separate values if only one day was available) to reflect a more general diet. This study also excluded samples without smoking status since many researchers have agreed that smoking has a significant impact on the effects of caffeine on blood pressure [2,7].
Since previous studies have suggested that there is a high probability of a nonlinear relationship between caffeine and blood pressure [2,4], nonlinear regression models with restrictive cubic spline were used to find the relationship between caffeine and hypertension adjusting by age, BMI, alcohol intake, sodium intake and sex. Considering that hypertension is a binary variable, logistic regression models were also used to analyze the relationship between caffeine intake and hypertension. Meanwhile, menopausal women are widely recognized to have a higher risk of high blood pressure [12-14]. A linear regression model for women over 50 years of age was used to analyze the relationship between caffeine intake and blood pressure. All analyses were done by using R version 4.4.1. All statistical tests were evaluated at an alpha level of 0.05.
3. Results
Table 1. Baseline characteristics of the study population by presence or absence of hypertension (N=5153)
Hypertension (N=965) | No Hypertension (N=4188) | Overall (N=5153) | P-value | |
Diastolic: Blood pressure (mm Hg) | ||||
Mean (SD) | 86.1 (12.3) | 70.1 (9.00) | 73.1 (11.5) | <0.001 |
Median [Min, Max] | 86.7 [44.0, 135] | 70.0 [38.0, 90.0] | 72.0 [38.0, 135] | |
Systolic: Blood pressure (mm Hg) | ||||
Mean (SD) | 152 (14.8) | 115 (12.0) | 122 (19.1) | <0.001 |
Median [Min, Max] | 149 [118, 219] | 115 [76.3, 140] | 119 [76.3, 219] | |
Caffeine Intake (mg) | ||||
Mean (SD) | 134 (143) | 121 (190) | 124 (183) | <0.001 |
Median [Min, Max] | 98.0 [0, 1140] | 72.0 [0, 4680] | 76.0 [0, 4680] | |
Age (years) | ||||
Mean (SD) | 60.8 (14.4) | 41.1 (20.4) | 44.8 (20.9) | <0.001 |
Median [Min, Max] | 63.0 [12.0, 80.0] | 40.0 [12.0, 80.0] | 46.0 [12.0, 80.0] | |
BMI (kg/m**2) | ||||
Mean (SD) | 30.4 (7.13) | 28.7 (7.48) | 29.0 (7.44) | <0.001 |
Median [Min, Max] | 29.2 [14.8, 64.2] | 27.6 [13.2, 74.8] | 27.9 [13.2, 74.8] | |
Alcohol Intake (gm) | ||||
Mean (SD) | 8.29 (25.0) | 5.96 (18.4) | 6.40 (19.8) | 0.002 |
Median [Min, Max] | 0 [0, 388] | 0 [0, 301] | 0 [0, 388] | |
Sodium Intake (mg) | ||||
Mean (SD) | 3250 (1590) | 3310 (1550) | 3300 (1560) | 0.122 |
Median [Min, Max] | 2960 [370, 12400] | 3080 [86.0, 25900] | 3070 [86.0, 25900] | |
Smoking | ||||
Yes | 194 (20.1%) | 797 (19.0%) | 991 (19.2%) | 0.748 |
No | 771 (79.9%) | 3391 (81.0%) | 4162 (80.8%) |
There were 5153 participants including 965 people with hypertension and 4188 people without it overall in this study. Table 1 provided statistical descriptions of multiple variables for both hypertension and non-hypertension groups, including diastolic blood pressure, systolic blood pressure, caffeine intake, age, body mass index, alcohol intake, sodium intake, and whether participants smoke. Comparing the characteristic distribution of hypertensive and non-hypertensive populations, the mean and median diastolic blood pressure and systolic blood pressure of hypertensive people were significantly higher than those of non-hypertensive people. Meanwhile, the mean and median caffeine intake and alcohol intake in the hypertensive group was also slightly higher than in the non-hypertension group, although the difference was not significant. And the mean age of the hypertensive group was significantly higher than that of the non-hypertension group, which is consistent with the theory that hypertension is usually age-related. The significant difference between the two groups was also seen in the BMI. Although studies have found a significant effect of sodium intake and smoking on hypertension, there was no significant difference between the mean and median values of sodium intake and smoking rate between the two groups.
Table 2. Restrictive cubic spline model results between blood pressure and caffeine intake
Systolic: Blood pressure (mm Hg) | Diastolic: Blood pressure (mm Hg) | |||
Characteristic | Beta1 | SE2 | Beta1 | SE2 |
Caffeine Intake (mg) | ||||
x | -0.172*** | 0.063 | -0.062 | 0.042 |
x2 | 132*** | 45.9 | 67.6** | 30.7 |
x3 | -138*** | 47.9 | -70.8** | 32.0 |
x4 | 6.56*** | 2.14 | 3.60** | 1.43 |
Age (years) | 0.501*** | 0.012 | 0.100*** | 0.008 |
BMI (kg/m**2) | 0.025 | 0.031 | 0.353*** | 0.021 |
Alcohol Intake (gm) | 0.063*** | 0.012 | 0.063*** | 0.008 |
Sodium Intake (mg) | 0.001*** | 0.000 | 0.000* | 0.000 |
Smoking | -1.21** | 0.596 | -2.26*** | 0.398 |
Sex | 0.372 | 0.456 | 0.035 | 0.305 |
No. Obs. | 5,153 | 5,153 | ||
Adjusted R² | 0.288 | 0.126 | ||
AIC | 43,307 | 39,148 | ||
1*p<0.1; **p<0.05; ***p<0.01 | ||||
2SE = Standard Error | ||||
3x = Caffeine Intake (mg) | ||||
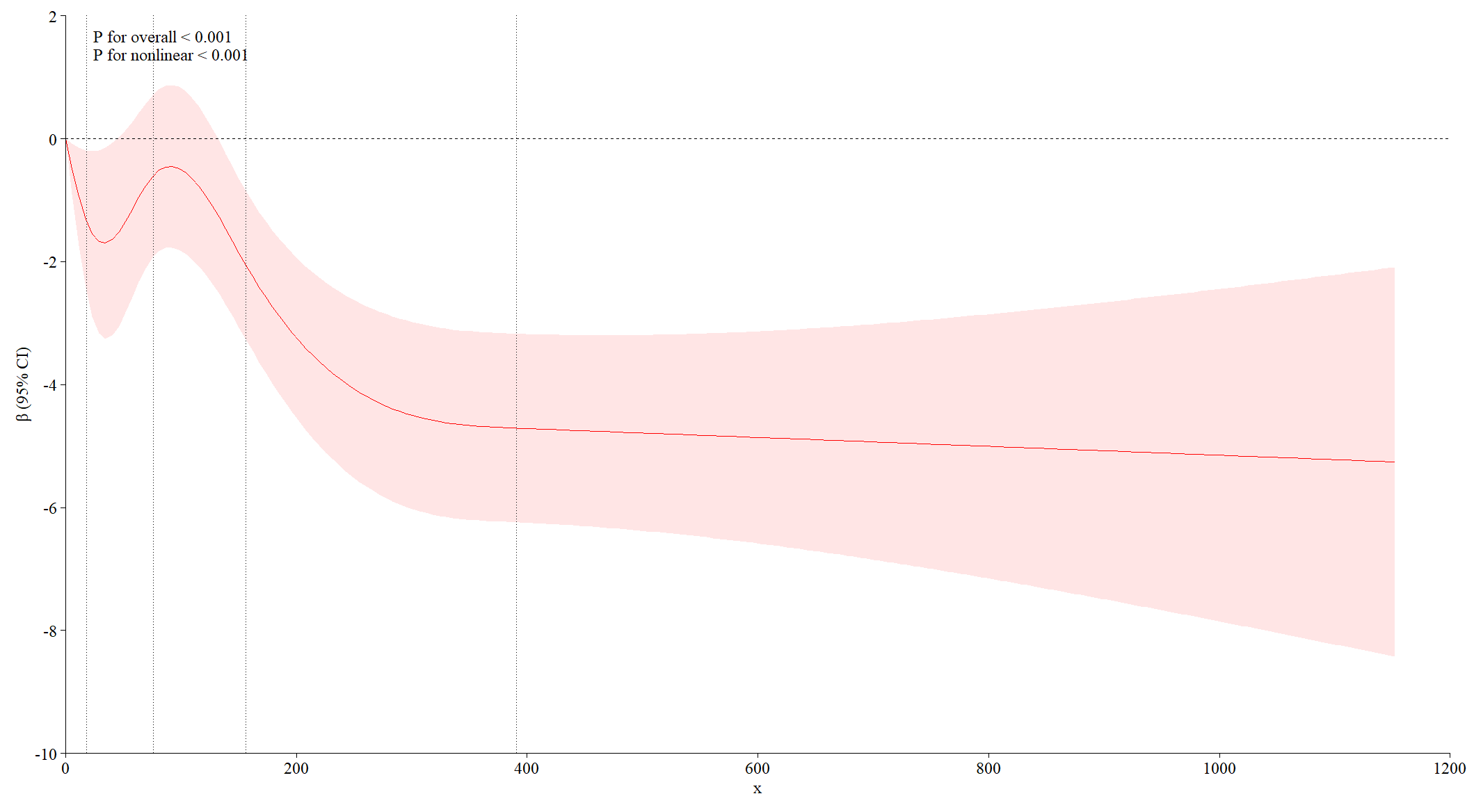
Figure 1. Coefficient of caffeine intake in systolic blood pressure
The vertical dashed lines represent the 0.05, 0.275, 0.5, 0.725, and 0.95 percentiles of caffeine intake, and their specific values are 0.0, 18.5, 76.0, 156.5, and 390.7 mg. Estimates were adjusted for age, BMI, alcohol intake, salt intake, smoking, and gender. The overall correlation p-value and nonlinear p-value were less than 0.001 for all outcomes.
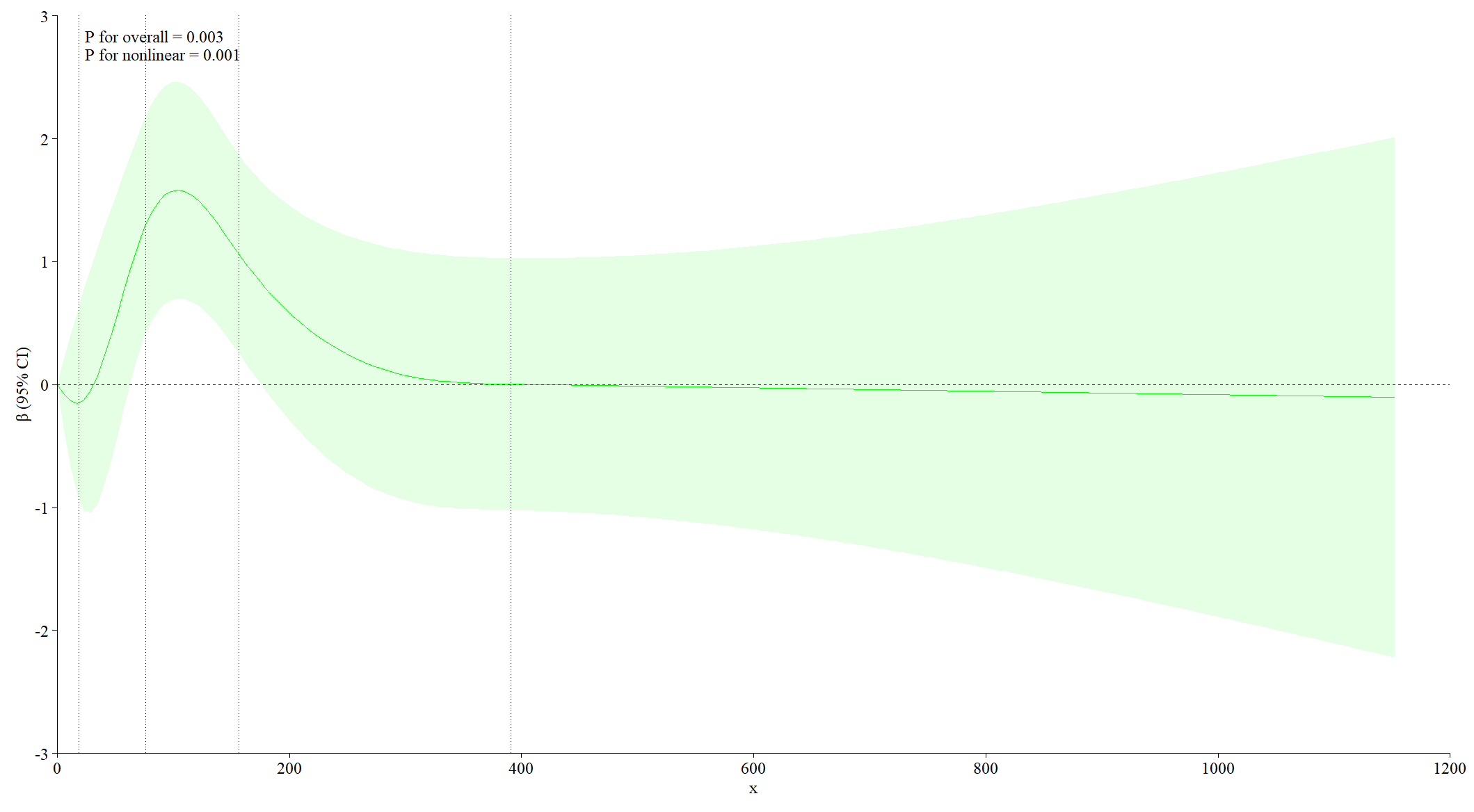
Figure 2. Coefficient of caffeine intake in diastolic blood pressure
The vertical dashed lines represent the 0.05, 0.275, 0.5, 0.725, and 0.95 percentiles of caffeine intake, and their specific values are 0.0, 18.5, 76.0, 156.5, and 390.7 mg. Estimates were adjusted for age, BMI, alcohol intake, salt intake, smoking, and gender. The overall correlation p-value was 0.003, and nonlinear p-value was 0.001.
The restrictive cubic spline model was used to observe a nonlinear relationship between caffeine intake and blood pressure. This study found that caffeine intake has a negative relationship with both systolic and diastolic blood pressure at caffeine intake below 18.5 mg, followed by a significant alternating positive and negative relationship (Figure 1, Figure 2). Although caffeine intake has the negative correlation with systolic blood pressure overall, a U-shaped relationship and an inverted U-shaped relationship also occur during the increase in caffeine intake (Figure 1). Caffeine intake was positively correlated with diastolic blood pressure over time as caffeine intake increased, although the effects fluctuated (Figure 2). This suggests that caffeine intake has a significant effect on both diastolic and systolic blood pressure, but the mechanisms of the effect are likely to be different.
Table 3. Logistic regression model results between hypertension and caffeine intake
Hypertension | ||
Characteristic | OR12 | SE2 |
Caffeine Intake (mg) | 0.999*** | 0.000 |
Age (years) | 1.06*** | 0.002 |
BMI (kg/m**2) | 1.02*** | 0.005 |
Alcohol Intake (gm) | 1.01*** | 0.002 |
Sodium Intake (mg) | 1.00* | 0.000 |
Sex | 1.05 | 0.079 |
Smoking | 0.736*** | 0.101 |
No. Obs. | 5,153 | |
AIC | 4,173 | |
BIC | 4,226 | |
1*p<0.1; **p<0.05; ***p<0.01 | ||
2OR = Odds Ratio, SE = Standard Error | ||
The first two models are about the relationship between caffeine intake and blood pressure, which intuitively reflects the effect of caffeine on blood pressure. In order to analyze the relationship between caffeine intake and risk of hypertension, a logistic regression model was introduced for analysis. We found that for every milligram increase in caffeine intake, the chance of developing hypertension was reduced by about 0.1% (Table 3). However, the effect was statistically significant (p<0.01), although the actual magnitude was small.
Table 4. Linear regression model results between blood pressure and caffeine intake in menopausal women
Systolic: Blood pressure (mm Hg) | Diastolic: Blood pressure (mm Hg) | ||||
Characteristic | Beta1 | SE2 | Beta1 | SE2 | |
Caffeine Intake (mg) | -0.00081 | 0.002 | -0.00263* | 0.001 | |
Age (years) | 0.35542*** | 0.031 | 0.36870*** | 0.023 | |
BMI (kg/m**2) | 0.07333* | 0.042 | 0.31918*** | 0.032 | |
Alcohol Intake (gm) | 0.07848*** | 0.019 | 0.06513*** | 0.014 | |
Sodium Intake (mg) | 0.00100*** | 0.000 | 0.00024 | 0.000 | |
Smoking | -1.6238** | 0.821 | -1.2657** | 0.623 | |
No. Obs. | 1,468 | 1,468 | |||
Adjusted R² | 0.155 | 0.297 | |||
AIC | 11,543 | 10,734 | |||
1*p<0.1; **p<0.05; ***p<0.01 | |||||
2SE = Standard Error | |||||
Several studies have shown that menopausal women are at high risk of hypertension [12-14], we subset our dataset and reproduce the same analysis. Consistent with the results of previous studies by Rhee et al. [10], there was no significant relationship between caffeine intake and blood pressure in menopausal women (Table 4).
4. Discussion
This study suggests that caffeine intake has a moderating effect on blood pressure and is associated with the risk of developing hypertension. This is consistent with the finding of Zhenzhen Zhang, et al. [15] that certain components of coffee have the effect of lowering blood pressure. Gaeini et al. [5] found that coffee contains a variety of bioactive compounds such as chlorogenic acid, caffeol and cafestol. They have antioxidant, anti-inflammatory and vasodilatory effects, affect nitric oxide synthesis, lipid metabolism and endothelial function [16,17], and can lower blood pressure. Among the metabolites of chlorogenic acids, ferulic acid is able to positively affect blood pressure by increasing the bioavailability of nitric oxide and by enhancing the endothelium-dependent vasodilatory effects induced by acetylcholine [18, 19]. Other factors included in the model, such as age, BMI, alcohol and sodium intake, can also raise blood pressure. For example, blood vessel elasticity decreases with age, leading to increased blood pressure [20]. There is also the fact that people with higher BMI are usually associated with obesity and metabolic disorders leading to hypertension. Additionally, we found a tendency for blood pressure to increase when a certain threshold was exceeded. This is related to the mechanism by which caffeine induces atherosclerosis by releasing norepinephrine and epinephrine which further cause vasoconstriction, thereby affecting vascular elasticity [21].
In order to make the final results more accurate, multiple studies have attempted large-scale data and scientific methods of analysis and incorporation of a number of confounding factors. We included age, sex, BMI, lifestyle and so on. Giuseppe et al [20] have also shown that these factors can influence blood pressure response to caffeine. Koksal et al. 's [9] study focused on age as a confounding factor, but also mentioned gender, BMI, waist circumference, smoking status and other factors that may be related to blood pressure. We recognize that the relationship between caffeine intake and hypertension is complex and can be influenced by a number of factors. In the selection of lifestyle confounding factors, we focused on smoking and alcohol consumption. Guessous et al. [22] also mention that smoking may affect the effect of coffee or caffeine on blood pressure. We analyzed it and got that caffeine has a moderating effect on blood pressure to some extent. And the results obtained by the meta of D'Elia et al. [4] are in line with ours to a certain extent. We also researched the effect of caffeine intake on systolic and diastolic blood pressure in menopausal women. Finally, it was concluded that caffeine intake in menopausal women was not associated with either blood pressure. This agrees with the findings of Rhee et al. [10].
Of course, there are many differences between us and other studies. We have some discrepancies compared to the findings of Köksal et al [9]. Our findings alternated between positive and negative correlations between caffeine intake and blood pressure values. But Köksal et al. noted positive correlation between caffeine and blood pressure. This may be due to differences in the study population and methods or other factors of the covariates considered. Our study population came from the NHANES database, whereas Chei et al. [2] chose a study population from the Singapore Chinese Health Cohort. The results may vary because the relationship between caffeine and blood pressure is influenced by different people's lifestyle, diet, genetic background and other factors. In conclusion, the assessment of caffeine intake in different studies is confounded by a number of factors. For example, blood pressure is not always measured in the same way.
There are some limitations to our study. First, there is the problem of under-representation of certain groups. The data used in our study came from NHANES. While the dataset is representative, it is not representative of the community as a whole. Moreover, we still have unconsidered covariates. Examples include individual genetic differences, dietary habits, and lifestyle. Lastly, we can't determine a causal relationship between caffeine and high blood pressure. Our study was conducted on observational data and the effect of confounding factors cannot be completely excluded. Therefore, our findings can only suggest an association between caffeine intake and hypertension. Our strength is that we used a non-linear model, which allows us to observe the relationship between caffeine intake and blood pressure values more comprehensively. We also analyzed specific populations. A subset of analyses was conducted for the high-risk group of menopausal women. This helps to provide more insight into the effect of caffeine on the risk of hypertension in different populations.
5. Conclusion
This study focused on the correlation between caffeine intake and risk of hypertension. The results present that caffeine has a modulating effect on blood pressure and is associated with the risk of developing hypertension. However, this study still has some limitations. For example, under representation of certain groups and the inability to establish a causal relationship between caffeine and hypertension. Currently, there is no basis to suggest that the adult population can prevent HPT by avoiding coffee consumption. Further research in this direction can be done in the future by incorporating more nuanced variables. It enables a better understanding of the relationship and its implications for public health and personal health management.
Author Contribution
All the authors contributed equally to this work and should be considered as co-first authors.
References
[1]. March 2023 WHO hypertension Key facts. https://www.who.int/news-room/fact-sheets/detail/hypertension
[2]. Chei, C.-L., Loh, J. K., Soh, A., Yuan, J.-M., & Koh, W.-P. (2018). Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. European Journal of Nutrition, 57(4), 1333–1342. https://doi.org/10.1007/s00394-017-1412-4
[3]. Klag, M. J., Wang, N.-Y., Meoni, L. A., Brancati, F. L., Cooper, L. A., Liang, K.-Y., Young, J. H., & Ford, D. E. (2002). Coffee Intake and Risk of Hypertension: The Johns Hopkins Precursors Study. Archives of Internal Medicine, 162(6), 657–662. https://doi.org/10.1001/archinte.162.6.657
[4]. D’Elia, L., Fata, E. L., Galletti, F., Scalfi, L., & Strazzullo, P. (2019). Coffee consumption and risk of hypertension: A dose–response meta-analysis of prospective studies. European Journal of Nutrition, 58(1), 271–280. https://doi.org/10.1007/s00394-017-1591-z
[5]. Gaeini, Z., Bahadoran, Z., Mirmiran, P., & Azizi, F. (2019). Tea, coffee, caffeine intake and the risk of cardio-metabolic outcomes: Findings from a population with low coffee and high tea consumption. Nutrition & Metabolism, 16(1), 28. https://doi.org/10.1186/s12986-019-0355-6
[6]. SPM, U. C., Monique, V. W., Bas, B.-M. H., Marga, O., M, G. J., C, B. H., HM, P. P., JM, F. E., & E, G. D. (2007). Coffee intake and incidence of hypertension. The American Journal of Clinical Nutrition, 85(3), 718–723. https://doi.org/10.1093/ajcn/85.3.718
[7]. Jinnie J, R., FeiFei, Q., K, H. H., I, C. T., E, B. C., Oleg, Z., E, M. J., L, S. M., & C, W. W. (2016). Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. The American Journal of Clinical Nutrition, 103(1), 210–217. https://doi.org/10.3945/ajcn.115.120147
[8]. Surma, S., & Oparil, S. (2021). Coffee and Arterial Hypertension. Current Hypertension Reports, 23(7), 38. https://doi.org/10.1007/s11906-021-01156-3
[9]. Eda Köksal, Hülya Yardımcı, Betül Kocaadam, Burcu Deniz Güneş, Birsen Yılmaz & Efsun Karabudak (2016) Relationship between dietary caffeine intake and blood pressure in adults. https://pubmed.ncbi.nlm.nih.gov/27589213/
[10]. Jinnie J Rhee, FeiFei Qin, Haley K Hedlin, Tara I Chang, Chloe E Bird, Oleg Zaslavsky, JoAnn E Manson, Marcia L Stefanick, and Wolfgang C Winkelmayer (2016) Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4691674/
[11]. Michael J. Klag, Nae-Yuh Wang, Lucy A. Meoni, Frederick L. Brancati, Lisa A. Cooper, Kung- Yee Liang, J. Hunter Young, Daniel E. Ford (2002) Coffee intake and the risk of hypertension. https://pubmed.ncbi.nlm.nih.gov/11911719/
[12]. Rosenthal, T., Oparil, S. Hypertension in women. J Hum Hypertens 14, 691–704 (2000). https://doi.org/10.1038/sj.jhh.1001095
[13]. Ong, K. L., Tso, A. W. K., Lam, K. S. L., & Cheung, B. M. Y. (2008). Gender Difference in Blood Pressure Control and Cardiovascular Risk Factors in Americans With Diagnosed Hypertension. Hypertension, 51(4), 1142–1148. https://doi.org/10.1161/HYPERTENSIONAHA.107.105205
[14]. Taddei, S. (2009). Blood pressure through aging and menopause. Climacteric. https://doi.org/10.1080/13697130903004758
[15]. Zhenzhen Zhang, Gang Hu, Benjamin Caballero, Lawrence Appel, and Liwei Chen. (2011). Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies,93:1212–9.
[16]. Emami, M.R.; Safabakhsh, M.; Alizadeh, S.; Asbaghi, O.; Khosroshahi, M.Z. Effect of vitamin E supplementation on blood pressure: A systematic review and meta-analysis. J. Hum. Hypertens. 2019, 33, 499–507. [CrossRef] [PubMed]
[17]. Zeman, M.; Vecka, M.; Perlík, F.; Sta ˇnková, B.; Hromádka, R.; Tvrzická, E.; Širc, J.; Hrib, J.; Žák, A. Pleiotropic effects of niacin:Current possibilities for its clinical use. Acta Pharm. 2016, 66, 449–469. [CrossRef]
[18]. Suzuki A, Kagawa D, Fujii A, Ochiai R, Tokimitsu I, Saito I (2002) Short- and long-term effects of ferulic acid on blood pressure in spontaneously hypertensive rats. Am J Hypertens 15:351–357
[19]. Suzuki A, Yamamoto M, Jokura H, Fujii A, Tokimitsu I, Hase T, Saito I (2207) Ferulic acid restores endothelium-dependent vasodilation in aortas of spontaneously hypertensive rats. Am J Hypertens 20:508–513
[20]. Rachele De Giuseppe, Ilaria Di Napoli, Francesca Granata, Antonia Mottolese, Hellas Cena (2019) Caffeine and blood pressure: a critical review perspective.Nutrition Research Reviews 32:169–175
[21]. Rodríguez-Artalejo, F.; López-García, E. Coffee Consumption and Cardiovascular Disease: A Condensed Review of Epidemiological Evidence and Mechanisms. J. Agric. Food Chem. 2018, 66, 5257–5263. [CrossRef] [PubMed]
[22]. Idris Guessous & Chin B. Eap & Murielle Bochud. (2014). Blood Pressure in Relation to Coffee and Caffeine Consumption.16:468
Cite this article
Yang,R.;Fan,Y.;Jin,T. (2025). The Correlation between Caffeine Intake and the Risk of Hypertension. Theoretical and Natural Science,78,85-94.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 4th International Conference on Biological Engineering and Medical Science
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. March 2023 WHO hypertension Key facts. https://www.who.int/news-room/fact-sheets/detail/hypertension
[2]. Chei, C.-L., Loh, J. K., Soh, A., Yuan, J.-M., & Koh, W.-P. (2018). Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. European Journal of Nutrition, 57(4), 1333–1342. https://doi.org/10.1007/s00394-017-1412-4
[3]. Klag, M. J., Wang, N.-Y., Meoni, L. A., Brancati, F. L., Cooper, L. A., Liang, K.-Y., Young, J. H., & Ford, D. E. (2002). Coffee Intake and Risk of Hypertension: The Johns Hopkins Precursors Study. Archives of Internal Medicine, 162(6), 657–662. https://doi.org/10.1001/archinte.162.6.657
[4]. D’Elia, L., Fata, E. L., Galletti, F., Scalfi, L., & Strazzullo, P. (2019). Coffee consumption and risk of hypertension: A dose–response meta-analysis of prospective studies. European Journal of Nutrition, 58(1), 271–280. https://doi.org/10.1007/s00394-017-1591-z
[5]. Gaeini, Z., Bahadoran, Z., Mirmiran, P., & Azizi, F. (2019). Tea, coffee, caffeine intake and the risk of cardio-metabolic outcomes: Findings from a population with low coffee and high tea consumption. Nutrition & Metabolism, 16(1), 28. https://doi.org/10.1186/s12986-019-0355-6
[6]. SPM, U. C., Monique, V. W., Bas, B.-M. H., Marga, O., M, G. J., C, B. H., HM, P. P., JM, F. E., & E, G. D. (2007). Coffee intake and incidence of hypertension. The American Journal of Clinical Nutrition, 85(3), 718–723. https://doi.org/10.1093/ajcn/85.3.718
[7]. Jinnie J, R., FeiFei, Q., K, H. H., I, C. T., E, B. C., Oleg, Z., E, M. J., L, S. M., & C, W. W. (2016). Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. The American Journal of Clinical Nutrition, 103(1), 210–217. https://doi.org/10.3945/ajcn.115.120147
[8]. Surma, S., & Oparil, S. (2021). Coffee and Arterial Hypertension. Current Hypertension Reports, 23(7), 38. https://doi.org/10.1007/s11906-021-01156-3
[9]. Eda Köksal, Hülya Yardımcı, Betül Kocaadam, Burcu Deniz Güneş, Birsen Yılmaz & Efsun Karabudak (2016) Relationship between dietary caffeine intake and blood pressure in adults. https://pubmed.ncbi.nlm.nih.gov/27589213/
[10]. Jinnie J Rhee, FeiFei Qin, Haley K Hedlin, Tara I Chang, Chloe E Bird, Oleg Zaslavsky, JoAnn E Manson, Marcia L Stefanick, and Wolfgang C Winkelmayer (2016) Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4691674/
[11]. Michael J. Klag, Nae-Yuh Wang, Lucy A. Meoni, Frederick L. Brancati, Lisa A. Cooper, Kung- Yee Liang, J. Hunter Young, Daniel E. Ford (2002) Coffee intake and the risk of hypertension. https://pubmed.ncbi.nlm.nih.gov/11911719/
[12]. Rosenthal, T., Oparil, S. Hypertension in women. J Hum Hypertens 14, 691–704 (2000). https://doi.org/10.1038/sj.jhh.1001095
[13]. Ong, K. L., Tso, A. W. K., Lam, K. S. L., & Cheung, B. M. Y. (2008). Gender Difference in Blood Pressure Control and Cardiovascular Risk Factors in Americans With Diagnosed Hypertension. Hypertension, 51(4), 1142–1148. https://doi.org/10.1161/HYPERTENSIONAHA.107.105205
[14]. Taddei, S. (2009). Blood pressure through aging and menopause. Climacteric. https://doi.org/10.1080/13697130903004758
[15]. Zhenzhen Zhang, Gang Hu, Benjamin Caballero, Lawrence Appel, and Liwei Chen. (2011). Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies,93:1212–9.
[16]. Emami, M.R.; Safabakhsh, M.; Alizadeh, S.; Asbaghi, O.; Khosroshahi, M.Z. Effect of vitamin E supplementation on blood pressure: A systematic review and meta-analysis. J. Hum. Hypertens. 2019, 33, 499–507. [CrossRef] [PubMed]
[17]. Zeman, M.; Vecka, M.; Perlík, F.; Sta ˇnková, B.; Hromádka, R.; Tvrzická, E.; Širc, J.; Hrib, J.; Žák, A. Pleiotropic effects of niacin:Current possibilities for its clinical use. Acta Pharm. 2016, 66, 449–469. [CrossRef]
[18]. Suzuki A, Kagawa D, Fujii A, Ochiai R, Tokimitsu I, Saito I (2002) Short- and long-term effects of ferulic acid on blood pressure in spontaneously hypertensive rats. Am J Hypertens 15:351–357
[19]. Suzuki A, Yamamoto M, Jokura H, Fujii A, Tokimitsu I, Hase T, Saito I (2207) Ferulic acid restores endothelium-dependent vasodilation in aortas of spontaneously hypertensive rats. Am J Hypertens 20:508–513
[20]. Rachele De Giuseppe, Ilaria Di Napoli, Francesca Granata, Antonia Mottolese, Hellas Cena (2019) Caffeine and blood pressure: a critical review perspective.Nutrition Research Reviews 32:169–175
[21]. Rodríguez-Artalejo, F.; López-García, E. Coffee Consumption and Cardiovascular Disease: A Condensed Review of Epidemiological Evidence and Mechanisms. J. Agric. Food Chem. 2018, 66, 5257–5263. [CrossRef] [PubMed]
[22]. Idris Guessous & Chin B. Eap & Murielle Bochud. (2014). Blood Pressure in Relation to Coffee and Caffeine Consumption.16:468