






1. Introduction
The ankle joint complex, which is made up of the distal tibiofibular joint, the talocrural joint, and the subtalar joint, functions as a vital contact between the foot and lower leg. Each of them contributes uniquely to the balance of mobility and stability required for locomotion. The TCJ is a hinge-type synovial joint. It connects the tibia (Tib), fibula (Fib), and talus, allowing for DF and PF. The STJ, consisting of anterior and posterior articulations between the calcaneus and talus, which allows eversion and inversion. Stabilization of these joints relies on ligamentous structures, including the deltoid ligament (DL), the lateral collateral ligaments (LCL), and the medial collateral ligament (MCL). Syndesmotic ligaments in the distal tibiofibular joint also play a vital role in stabilizing the fibula and tibia by firmly connecting them.
The biomechanical efficiency of the AJC is crucial for human locomotion. Gait mechanics rely heavily on the contribution of the plantar flexor muscles [1], which generate propulsion during the ankle push-off phase. This phase not only accelerates the center of mass but also facilitates the transition of the leg into the swing phase. The power generated by ankle push-off is essential for increasing the speed of the push-off limb [2]. The static and dynamic stabilizers of the ankle ensure proper motion and minimize the risk of ankle injuries in a normal gait cycle. A study showed that ankle injuries were most prevalent in 24 out of 70 sports, with ankle sprains being the most frequent injury in 33 out of 43 sports that involved ankle injuries. [3]. Specifically, up to 80% of all ankle injuries occurred at the lateral ankle ligaments [4]. Ankle sprains in athletes are often attributed to factors such as anatomic misalignment, inadequate physical conditioning, and improper technique. Additionally, external factors such as playing surface, weather conditions, and the level of athletic performance further influence the likelihood of injury [5].
2. Anatomy (Joints and Muscles)
The talus of the foot is connected to the tibia and fibula of the lower leg through the TCJ. The TCJ, the
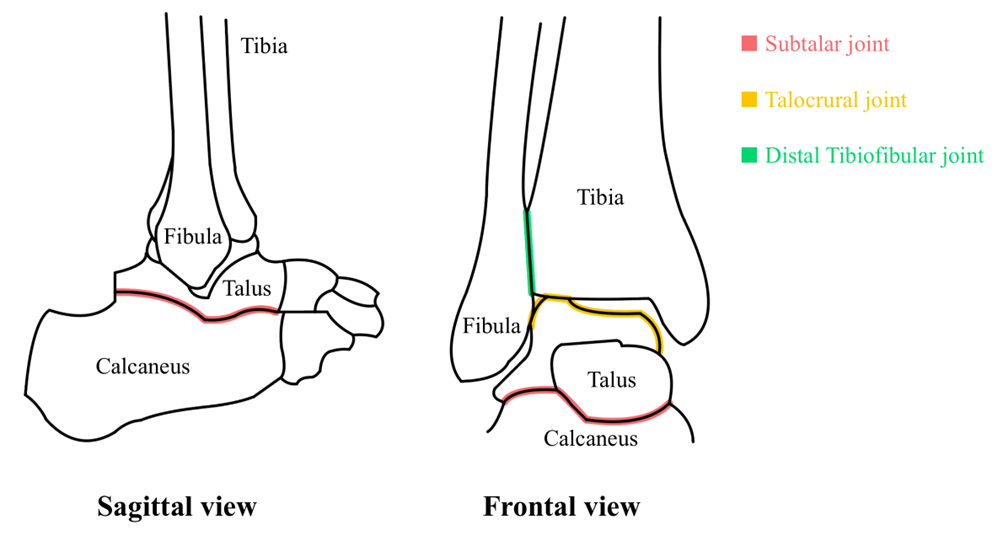
Figure 1: The diagram of three joints of ankle joint complex.
The STJ, sometimes referred to as the talocalcaneal joint, is an essential connection between the talus and calcaneus bones in the foot. The calcaneus, the biggest and most powerful bone in the foot, provides support for the movement of weight from the leg to the ground. The talus is located on the anterior part of the calcaneus. The posterior STJ was formed by the articulation of the inferior posterior facet of the calcaneus with the superior posterior facet of the talus [6]. The convex and concave facets of the STJ allow eversion and inversion of the ankle. Although other movements are possible at this point, it mainly allows the EV and IV of the foot [7]. The STJ is stabilized by several ligaments, including the medial and lateral talocalcaneal ligaments, the interosseous talocalcaneal ligament, and the cervical ligament. The ITL extends from the articular facets of the inferior talus to the superior surface of the calcaneus, serves as the primary connection between these two bones [8]. The cervical ligament is positioned anteriorly and laterally relative to the interosseous ligament, playing a crucial role in stabilizing both the anterior and posterior STJ. As the strongest ligament in the subtalar ligaments, it has been demonstrated to resist supination during in vitro kinematic studies [9].
The TCJ connects the talus bone of the foot to the lower ends of the tibia and fibula. It plays a crucial role in allowing dorsiflexion and plantar flexion, enabling movement such as lifting and lowering the foot. The TCJ is stabilized by the joint capsule and ligaments, such as the MCL and LCL. The anterior and posterior tibiotalar ligaments, the tibionavicular ligament, and the tibiocalcaneal ligament make up the DL, which supports the medial side of the joint. It plays a critical role in resisting EV movements and valgus stresses on the joint. On the lateral side, the lateral collateral ligaments limit joint inversion, reducing varus stress and controlling rotational forces [8]. These ligaments consist of the calcaneofibular ligament and the anterior and posterior talofibular ligaments. The stability of the lateral TCJ is ensured by the anterior and posterior talofibular ligaments, which are especially crucial in withstanding significant tensile pressures during DF and PF, respectively.
The stability of the AJC depends on the distal tibiofibular joint, which permits restricted movement between the fibula and tibia. It is a type of fibrous joint known as a syndesmosis, where two parallel bones are joined by ligaments or connective tissue. The distal fibula and tibia are connected and stabilized by the anterior and posterior inferior tibiofibular ligaments, along with the interosseous and the transverse ligaments. These syndesmotic ligaments restrain the fibula as it rotates externally and translates posteriorly with the tibia, thus stabilizing the ankle.
Most of the foot and ankle movements are generated by twelve extrinsic muscles which are categorized into four groups based on their location and function. These muscles originate from the leg and insert into the foot. The anterior muscles are comprised of the extensor hallucis longus, the extensor digitorum longus, the tibialis anterior, and the peroneus tertius [8]. The peroneus tertius facilitates both DF and EV of the foot, whereas the extensor digitorum longus contributes solely to DF. The other two muscles produce inversion and dorsiflexion. The posterior group can be divided into deep and superficial layers. The superficial layer is made of gastrocnemius, the plantaris, and the soleus, produces plantar flexion of the foot. The tibialis posterior, the flexor hallucis longus, and the flexor digitorum longus are the three muscles that make up the deep posterior group, which help with PF and foot inversion. The lateral muscles, the fibularis longus and brevis, produce PF and EV.
3. Motion of the ankle and foot
The major motion at the AJC is PF and DF in the sagittal plane, IV and EV in the frontal plane, abduction and abduction in the transverse plane. Supination and pronation are three-dimensional movements at both the STJ and TCJ, resulting from a combination of these motions. The AJC's axis of rotation differs across the three planes [8]. In the sagittal plane, it aligns with a line connecting the medial and lateral malleoli. In the coronal plane, the axis rotates around the intersection of the malleoli and the tibia's long axis in the frontal plane. In the transverse plane, the axis rotates along the tibia's long axis, intersecting the foot's midline. While simultaneous motions have been observed at the TCJ, this had been thought to result from its oblique axis [11]. Like the TCJ, an oblique axis also extends from posterior to anterior at the STJ. One study also found that the axes for plantar flexion, dorsiflexion, pronation, supination, and medial-lateral rotation converge or align closely near a central point within the talus's trochlea, regardless of their inclination [12].
4. Range of motion
Ankle movements primarily occur in the sagittal plane, with dorsiflexion and plantar flexion largely occurring at the TCJ. The ROM in the sagittal plane ranges approximately 65 to 75°, comprising 10 to 20° of DF and 40 to 55° of PF. In the frontal plane, the ankle joint complex exhibits about 35° of total ROM, including 23° of inversion and 12° of eversion [8]. However, these values can vary based on factors such as age, gender, and individual biomechanics. Research has shown that both gender and age significantly influence the range of motion in the AJC. Females aged from 9 to 20 years generally have a greater ankle ROM than males of the same age. Nonetheless, ROM begins to consistently decrease from the ages of 17 to 20, reaching its minimum after 60 in both genders; while females tend to have a greater average decline in ROM compared to males [13]. The ankle range of motion is also closely associated with ankle injury risk, particularly among athletes. Loss of ankle ROM is one of the risk factors for the recurrence of ankle injuries among sports population. Study indicates significant differences in the DF and PF range of motion of the ankle of the injured limb and sound limb. Ankle sprain limits ankle movements by causing stiffness and tightness [14]. Ankle injury risk is also strongly correlated with ankle ROM, especially in athletes. Study suggested that young female athletes have a greater plantar flexion and inversion ankle ROM than males, which potentially contributing to the higher proportion of ankle injury history in females. Since the most common ankle injuries, the lateral ankle sprain, mostly occur within the plantar flexion and inversion positions [15].
Different sports impose varying demands on the ankle range of motion, depending on their movement patterns and biomechanical needs. Unlike gymnastics which require high ankle ROM for flexibility and multidirectional agility, sports involving sprinting require less ankle ROM, prioritizing joint stiffness and stability to improve power output and efficiency. As the ankle range of motion increases, the relative peak power in both dominant and non-dominant limbs decreases. Research found that greater ankle ROM is associated with decreased power during the Running Anaerobic Sprint Test. As high ankle stiffness was believed to be associated with increased ground reaction forces, velocity, and efficiency in sprinting [16].
5. Conclusion
The ankle joint complex is a specialized structure designed to balance stability and mobility for various activities. Its function depends on the coordination of joint anatomy, muscles and ligaments. Variability in range of motion, influenced by factors such as age, gender, and sport-specific demands, which potentially underscores the importance of individualized approaches to training and rehabilitation. Future research should continue to explore the dynamic interactions within this complex system to further optimize outcomes for athletes and individuals.
References
[1]. Winter, D. A. (1983). Energy generation and absorption at the ankle and knee during fast, natural, and slow cadences. Clinical Orthopaedics and Related Research (1976-2007), 175, 147-154.
[2]. Zelik, K. E., & Adamczyk, P. G. (2016). A unified perspective on ankle push-off in human walking. Journal of Experimental Biology, 219(23), 3676-3683.
[3]. Fong, D. T. P., Hong, Y., Chan, L. K., Yung, P. S. H., & Chan, K. M. (2007). A systematic review on ankle injury and ankle sprain in sports. Sports medicine, 37, 73-94.
[4]. Mitchell, A., Dyson, R., Hale, T., & Abraham, C. (2008). Biomechanics of ankle instability. Part 2: Postural sway-reaction time relationship. Medicine and science in sports and exercise, 40(8), 1522-1528.
[5]. O’Loughlin, P. F., Murawski, C. D., Egan, C., & Kennedy, J. G. (2009). Ankle Instability in Sports. The Physician and Sportsmedicine, 37(2), 93–103. https://doi.org/10.3810/psm.2009.06.1715
[6]. Hertel J. (2002). Functional Anatomy, Pathomechanics, and Pathophysiology of Lateral Ankle Instability. Journal of athletic training, 37(4), 364–375.
[7]. Michael, J. M., Golshani, A., Gargac, S., & Goswami, T. (2008). Biomechanics of the ankle joint and clinical outcomes of total ankle replacement. Journal of the Mechanical Behavior of Biomedical Materials, 1(4), 276-294. https://doi.org/10.1016/j.jmbbm.2008.01.005
[8]. Brockett, C. L., & Chapman, G. J. (2016). Biomechanics of the ankle. Orthopaedics and Trauma, 30(3), 232-238. https://doi.org/10.1016/j.mporth.2016.04.015
[9]. Viladot, A., Lorenzo, J. C., Salazar, J., & Rodriguez, A. (1984). The subtalar joint: embryology and morphology. Foot & ankle, 5(2), 54-66.
[10]. Hermans, J. J., Beumer, A., De Jong, T. A., & Kleinrensink, G. J. (2010). Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. Journal of anatomy, 217(6), 633-645.
[11]. HICKS J. H. (1953). The mechanics of the foot. I. The joints. Journal of anatomy, 87(4), 345–357.
[12]. Lundberg, A., Svensson, O. K., Nemeth, G., & Selvik, G. (1989). The axis of rotation of the ankle joint. The Journal of Bone & Joint Surgery British Volume, 71(1), 94-99.
[13]. Grimston, S. K., Nigg, B. M., Hanley, D. A., & Engsberg, J. R. (1993). Differences in ankle joint complex range of motion as a function of age. Foot & ankle, 14(4), 215-222.
[14]. Alomar, A. I., Nuhmani, S., Ahsan, M., & Muaidi, Q. I. (2023). A comparison of the range of motion and dynamic stability of the ankle joint of athletes with an ankle sprain as compared to healthy controls: A cross-sectional study. International Journal of Critical Illness and Injury Science, 13(3), 138–144. https://doi.org/10.4103/ijciis.ijciis_2_23
[15]. Sugimoto, D., McCartney, R. E., Parisien, R. L., Dashe, J., Borg, D. R., & Meehan, W. P. (2018). Range of motion and ankle injury history association with sex in pediatric and adolescent athletes. The Physician and Sportsmedicine, 46(1), 24–29. https://doi.org/10.1080/00913847.2018.1413919
[16]. Wilson, S. J., Diaz, D. C., Young, T., DeJohn, D., Horsfall, C., Munkasy, B., Li, L., Rossi, S., & Mutchler, J. A. (2024). Association Between Ankle Range Of Motion And Anaerobic Sprint Test Performance In American Professional Soccer: 614. Medicine and Science in Sports and Exercise, 56(10S), 201–201. https://doi.org/10.1249/01.mss.0001054280.34555.6a
Cite this article
Lin,S. (2025). Biomechanics of the Ankle. Theoretical and Natural Science,91,18-22.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of ICMMGH 2025 Symposium: Computational Modelling in Biology and Medicine
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Winter, D. A. (1983). Energy generation and absorption at the ankle and knee during fast, natural, and slow cadences. Clinical Orthopaedics and Related Research (1976-2007), 175, 147-154.
[2]. Zelik, K. E., & Adamczyk, P. G. (2016). A unified perspective on ankle push-off in human walking. Journal of Experimental Biology, 219(23), 3676-3683.
[3]. Fong, D. T. P., Hong, Y., Chan, L. K., Yung, P. S. H., & Chan, K. M. (2007). A systematic review on ankle injury and ankle sprain in sports. Sports medicine, 37, 73-94.
[4]. Mitchell, A., Dyson, R., Hale, T., & Abraham, C. (2008). Biomechanics of ankle instability. Part 2: Postural sway-reaction time relationship. Medicine and science in sports and exercise, 40(8), 1522-1528.
[5]. O’Loughlin, P. F., Murawski, C. D., Egan, C., & Kennedy, J. G. (2009). Ankle Instability in Sports. The Physician and Sportsmedicine, 37(2), 93–103. https://doi.org/10.3810/psm.2009.06.1715
[6]. Hertel J. (2002). Functional Anatomy, Pathomechanics, and Pathophysiology of Lateral Ankle Instability. Journal of athletic training, 37(4), 364–375.
[7]. Michael, J. M., Golshani, A., Gargac, S., & Goswami, T. (2008). Biomechanics of the ankle joint and clinical outcomes of total ankle replacement. Journal of the Mechanical Behavior of Biomedical Materials, 1(4), 276-294. https://doi.org/10.1016/j.jmbbm.2008.01.005
[8]. Brockett, C. L., & Chapman, G. J. (2016). Biomechanics of the ankle. Orthopaedics and Trauma, 30(3), 232-238. https://doi.org/10.1016/j.mporth.2016.04.015
[9]. Viladot, A., Lorenzo, J. C., Salazar, J., & Rodriguez, A. (1984). The subtalar joint: embryology and morphology. Foot & ankle, 5(2), 54-66.
[10]. Hermans, J. J., Beumer, A., De Jong, T. A., & Kleinrensink, G. J. (2010). Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. Journal of anatomy, 217(6), 633-645.
[11]. HICKS J. H. (1953). The mechanics of the foot. I. The joints. Journal of anatomy, 87(4), 345–357.
[12]. Lundberg, A., Svensson, O. K., Nemeth, G., & Selvik, G. (1989). The axis of rotation of the ankle joint. The Journal of Bone & Joint Surgery British Volume, 71(1), 94-99.
[13]. Grimston, S. K., Nigg, B. M., Hanley, D. A., & Engsberg, J. R. (1993). Differences in ankle joint complex range of motion as a function of age. Foot & ankle, 14(4), 215-222.
[14]. Alomar, A. I., Nuhmani, S., Ahsan, M., & Muaidi, Q. I. (2023). A comparison of the range of motion and dynamic stability of the ankle joint of athletes with an ankle sprain as compared to healthy controls: A cross-sectional study. International Journal of Critical Illness and Injury Science, 13(3), 138–144. https://doi.org/10.4103/ijciis.ijciis_2_23
[15]. Sugimoto, D., McCartney, R. E., Parisien, R. L., Dashe, J., Borg, D. R., & Meehan, W. P. (2018). Range of motion and ankle injury history association with sex in pediatric and adolescent athletes. The Physician and Sportsmedicine, 46(1), 24–29. https://doi.org/10.1080/00913847.2018.1413919
[16]. Wilson, S. J., Diaz, D. C., Young, T., DeJohn, D., Horsfall, C., Munkasy, B., Li, L., Rossi, S., & Mutchler, J. A. (2024). Association Between Ankle Range Of Motion And Anaerobic Sprint Test Performance In American Professional Soccer: 614. Medicine and Science in Sports and Exercise, 56(10S), 201–201. https://doi.org/10.1249/01.mss.0001054280.34555.6a