






1. Introduction
The modern universal healthcare system, first developed in Germany, is primarily publicly funded, which the funding is collected from social insurance payments, and covers the full continuum of essential health services. It is observed that the universal healthcare system provides equitable and comprehensive access to health services improving population health, but it requires well-developed healthcare and economic system for the government. As population health has been brought to attention in recent decades, most developed countries started their universal healthcare system between 1950 and 1980.
Unlike most developed countries in Europe, the United States has become the most super-powered country in the world since WWII, but the government does not indicate to support the universal healthcare system. There are three important reasons the United States does not have a universal healthcare system: (1) Americans are more likely to be individualistic, believing healthcare for the sick is an individual’s responsibility than the government’s [1]. (2) Private healthcare businesses are the predominant sources in the United States, opposing universal healthcare to protect their profits and market share. (3) James Madison's Constitution was built on the idea that there shouldn't be a large redistribution of wealth from the wealthiest to the poor and middle-class residents in the country [2].
This study investigates the advantages and disadvantages of both universal and private healthcare systems, helping policymakers make decisions on health policy to improve the overall health of a country.
2. Analysis of the healthcare industry in the US
2.1. Hospitalization
The United States has one of the highest costs of healthcare in the world, in which the cost of illness could be twice as much as those of many other developed countries. However According to the Healthcare System Performance Rankings report, healthcare performance factors including care access, equity, outcome, and administrative efficiency in the United States were ranked last among the 11 countries [3], shown in Table 1. The low performance of these factors is primarily caused by the business monopoly and complex structure in the private-predominated healthcare system.
Table 1. Healthcare system performance rankings [3].
AUS | CAN | FRA | GER | NETH | NZ | NOR | SWE | SWIZ | UK | US | |
Overall Ranking | 3 | 10 | 8 | 5 | 2 | 6 | 1 | 7 | 9 | 4 | 11 |
Access to Care | 8 | 9 | 7 | 3 | 1 | 5 | 2 | 6 | 10 | 4 | 11 |
Care Process | 6 | 4 | 10 | 9 | 3 | 1 | 8 | 11 | 7 | 5 | 2 |
Administrative Efficiency | 2 | 7 | 6 | 9 | 8 | 3 | 1 | 5 | 10 | 4 | 11 |
Equity | 1 | 10 | 7 | 2 | 5 | 9 | 8 | 6 | 3 | 4 | 11 |
Health care Outcomes | 1 | 10 | 6 | 7 | 4 | 8 | 2 | 5 | 3 | 9 | 11 |
2.2. Monopoly in the healthcare system
In the United States, industry monopoly has become a major problem in the healthcare system, leading to high costs and low quality of medical services. Approximately 80% of hospitals are controlled by private nonprofit or for-profit organizations and most of those hospitals are owned by a few huge health systems. Unlike most other industries, the healthcare industry has higher entry barriers for new businesses. With fewer competitors in the market, those hospitals are usually operated by a few health systems in a geographic area, therefore, business consolidation and collaboration would appear. As a result, those health systems would be able to collaborate with each other and set their own price for the treatment regardless of the service quality, and patients have to suffer those burdens as there are no other options for them in the same geographic area.
A study analyzing the merger of two hospitals in Santa Cruz, California indicates that prices of the entire healthcare service rose dramatically after the merger over time in the Santa Cruz area [4]. When the market diverges from perfect competition due to the merger of existing companies, the new company gains the power to increase the prices by reducing the quantity. As a result, the price of the merged hospital in Santa Cruz rose about 23%. To react to the market equilibrium change, the competitor hospital in Santa Cruz also rose their prices by about 17 percent [4]. Although the prices increase in the market, the service quality does not necessarily need to be improved due to the supply shortage of medical services, and sometimes the service quality may be even worse than that before the merger. According to this study, it can be observed that monopoly in the United States healthcare industry has become a major problem negatively affecting healthcare performance in access, equity, and outcome driven by the high costs of illness and poor service quality.
In a universal health system, public care providers usually dominate the market, creating a healthier market environment. As the primary goal of the government is to increase population health, public-operated care providers may provide better services at lower prices. A good example could be found in the Chinese healthcare system. In China, the majority of hospitals are operated by the government which provides very affordable prices with national health insurance coverage for general treatments. In addition, the Chinese government allows the private sector to enter the healthcare field, but due to the intense pricing competition, they must perform much better than the public sector to survive in the industry.
2.3. Complex healthcare structure
The privately dominated healthcare industry in the United States also generates another obstruction of care access, which is the complexity of the healthcare structure. The nonlinear interactions of its components are essential to the success of this complex system, but self-organized parties in the healthcare system pay relatively little attention to patient enrollment, transitions, and communication channels [5]. The multiple systems and stakeholders are the major causes of the complexity of the healthcare structure in the United States. There are separate rules, funding, and costs associated with the different types of health insurance, such as employer-based, private insurance, or government-funded plans. The variety of health plans not only drives up the administration costs but also creates integration obstructions for patients to access care.
The insurance referral and approval processes are the major causes of making care access complicated due to service availability and multi-sector integration. In most cases, patients need to either request a referral or preauthorization from their primary doctors or get transferred to a third-party insurance contractor before surgery or specialty services. For example, if a patient is looking for hearing benefits through health insurance, he or she would need to reach out to the health plan or primary doctor to get a referral. The patient is most likely to be transferred to a third-party hearing insurance vendor to schedule a hearing test with the in-network audiologist or ENT. The entire process may take days to weeks depending on the availability of the provider and processing speed of the insurance eligibility files. On the one hand, most of those specialty services are handled by private providers, however, their availabilities have become a major problem delaying the treatment. On the other hand, each insurance company has its own portal to deliver the eligibility file, which usually requires additional time and steps for insurance verification. Thus, the complex healthcare structure in the United States has become a major problem for hospitalization, affecting care access and outcomes.
Nevertheless, in the universal health system, there are usually only one or a few insurance payers, which makes the entire process easier. When we study the Chinese healthcare system, there is only one health insurance payer, which is founded and operated by the government. All enrollees have a national health insurance card, which can be used for preventative service, purchasing medications, and hospitalization. Since the government manages the funds and integrations, all enrollees can easily access all of their local hospitals or pharmacies without preauthorization or claim approval. This procedure not only eliminates the unasserted waiting time but also reduces the administration cost significantly.
3. Analysis of the health insurance industry in the US
The complex health insurance system in the United States may cause delays affecting care access and outcome in hospitalization, however, there are many other health insurance-related problems with the private insurance system that impact people’s quality of life. The universal health coverage takes advantage of a nationwide funds pool and efficient administration process providing a cost-effective treatment method. However, the private insurance system does not only have a limited funds pool but also requires more workforce to service the system, thus, the overall costs would be higher than those of the universal health coverage system.
3.1. Funds pooling and coverage
There are approximately 1,000 insurance companies registered in the United States, in which their enrollee ranges from several hundred to nearly 49.5 million. According to the statistics, about 60% of the market shares are owned by the top 10 largest insurance companies (Figure 1). In this situation, the majority of those small insurance companies may not be able to provide comprehensive coverage to their enrollees because of the available funds and negotiation power. With less market share, small plans only have very limited funds collected from the insurance premium, thus, their coverage might be very limited depending on the treatment costs. Also, they have less negotiation power on price with the pharmaceutical companies and care providers as they have low demand for those treatment methods.
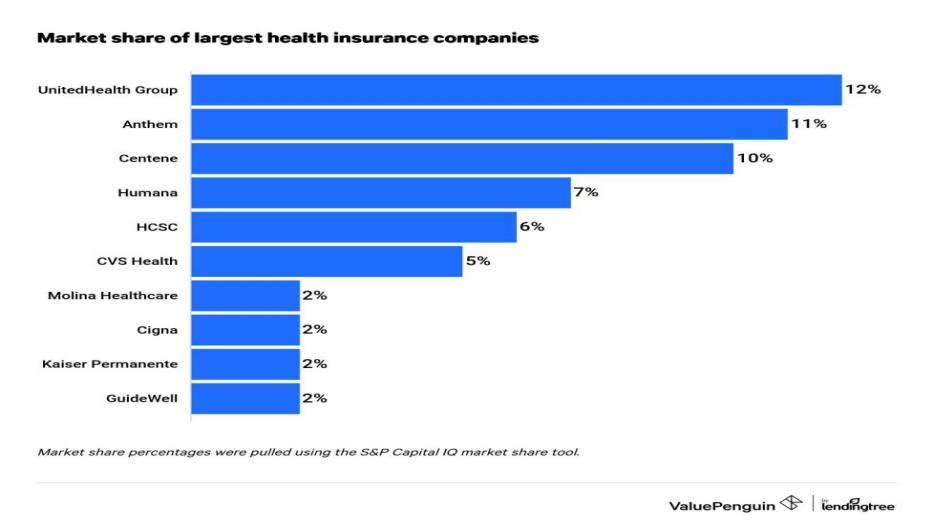
Figure 1. Market share of largest health insurance companies [6].
A good example can be found when comparing the orphan medicines coverage between the United States and those countries with universal coverage in Europe (Table 2). Most countries with universal health coverage in Europe usually have substantial reimbursement for orphan drugs and approve them according to their cost-effectiveness by national health institutions to ensure the money is spent efficiently. Germany, Italy, Sweden, and Norway have mostly full coverage, whereas Belgium, France, and Switzerland offer at least partial reimbursement for those orphan medicines [7]. However, the coverage decisions of orphan medicine in the United States are usually made by insurance companies according to cost-effectiveness upon their profit. According to a study, orphan medication coverage varies widely amongst plans. This finding has significant ramifications and indicates that a patient's insurance provider may affect their ability to obtain orphan medications. Plans most frequently impose patient subgroup limits in order to limit coverage of orphan medications. For instance, one plan limits the availability of omalizumab for the treatment of chronic idiopathic urticaria by mandating that patients have symptoms for at least 6 weeks prior to being approved for the medication. [8]. In addition, the high out-of-pocket cost of those orphan medicines may apply. Those restrictions on orphan medicines coverage in the United States could negatively impact care access and outcomes.
Table 2. Orphan medicines/rare diseases coverage and regulation by country [9].
Country | National Plan for Orphan Medicines | Reimbursement Process and/or Coverage; | HTA Criteria |
Belgium | Yes | Reimbursement decisions are made by the Ministry of Social Affairs and the Medical Advisory Council on orphan medicines | Therapeutic advantage, Budget Impact, and importance in clinical practice. |
France | Yes | Public social health insurance usually reimburses 60%-100%; Complementary health insurance often covers the remaining parts | Therapeutic advantage, unmet need, socio-economic benefits |
Germany | Yes | If no therapeutic alternative is available, public social health insurance automatically reimburses orphan medicines based on a cost-benefit analysis by IQWiG. Co-payment is limited to €10 per medicine and an annual threshold of 2% of individual yearly net income. | Cost-effectiveness |
Italy | Yes | Public social health insurance reimburses licensed orphan drugs through a standard pricing/reimbursement process (Law 658 and 5% AIFA special fund). | Cost-effectiveness, budget impact, need, existing therapies |
Sweden | Yes | The public social health insurance system handles reimbursement. The patient will receive the medications free of charge if the overall cost is more than 4300 SEK. | Cost-effectiveness, Human value, Solidarity |
Switzerland | No | Public social health insurance reimburses after a deductible and 10% co-payment (annual co-payment threshold of $646 USD). | Cost-effectiveness, Human value, Solidarity |
The United States | No | Medicare–approved health plans cover 95% after prior authorization and total “out of pocket” costs have exceeded $4350 USD. | Cost-effectiveness–No systematic HTA conducted by US payers for Orphan Drugs |
Furthermore, universal health coverage usually provides more comprehensive coverage to increase population health than those of private insurance. Achieving high coverage may help people live longer, be healthier, increase productivity, and experience fewer financial hardships connected to their health [10]. According to WHO–World Bank Index, those essential comprehensive coverages of universal health coverage have a significant impact on population health, especially for leading infectious causes of death, such as tuberculosis (TB), HIV/AIDS, and malaria (Table 3).
Table 3. Influence of Essential Services and The Justification of Universal Health Care System on Health [10].
Essential health service | Evidence of positive effects on health |
Family planning and care delivery | Reduced infant and maternal mortality |
Child immunization | Reduced mortality for children under 5 years old |
Pneumonia care | Reduced pneumonia-related morbidity and mortality |
Tuberculosis treatment | Reduced the prevalence of tuberculosis |
HIV antiretroviral therapy | Increased life expectancy, reduced HIV transmission |
Insecticide-treated bed nets for malaria prevention | Reduced malaria episodes and child mortality |
Access to basic sanitation | Reduced mortality and stunting of children under 5 years old |
Prevention and treatment of elevated blood pressure | Reduced all-cause mortality in individuals more than 60 years old, especially cardiovascular |
Prevention and treatment of elevated blood sugar | Reduced microvascular complications of diabetes, including kidney failure, loss of vision, and nerve damage |
Cervical cancer screening | Reduced cervical cancer incidence and mortality |
Basic hospital access | Reduced mortality caused by life-threatening emergencies |
Healthcare worker density | Improved overall health condition |
Access to essential medicines | Limiting the catastrophic healthcare costs |
3.2. Administration cost
One of the disadvantages of the private insurance system is the administration costs, which significantly increase the cost of healthcare. Similar to paying extra money when buying a house through a real estate agent, the United States government has to pay extra money “hiring” those private insurance companies providing service to their citizens. According to statistics, there are approximately 1,000 health and medical insurance companies with 563,366 people employed in the United States as of 2023 [11]. Those health insurance companies are more likely to be profit-driven businesses, gaining revenue from premiums and government support to satisfy salary. When we look into the salaries of health insurance CEOs in the United States, they range from $45,873 to $1,240,543, with a median salary of $224,106. The middle 57% of Health Insurance CEOs make between $224,117 and $562,687, with the top 86% making $1,240,543 [12]. A lot of health insurance funds are collected from enrollees and the government is paid for the administration rather than treatment.
A country with universal health coverage is more likely to have lower administration costs of health insurance than those in the United States because the government usually has direct control of the health insurance industry, effectively managing and handling all the insurance processes. A study comparing the administration cost of health insurance in the United States and Canada indicates that with a universal health insurance system, Canada has significantly lower administration costs of $307 per capita compared to $1,059 per capita in the United States in 1999 [13]. When examining the data analyzed in a study, we can observe that the health administration costs of each process in the United States are much higher than those in Canada (Figure 2). The high cost of health administration is a result of the complicated healthcare structure and profit-driven business.
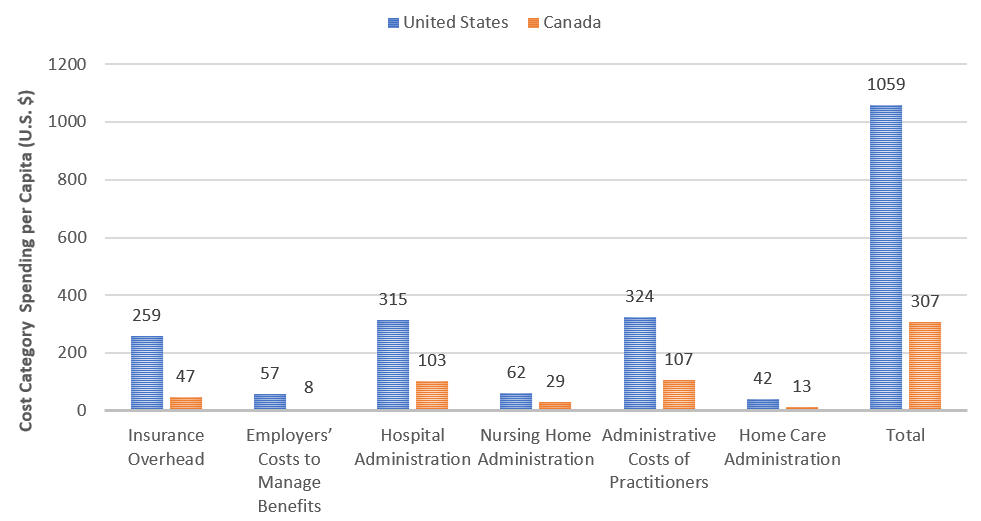
Figure 2. Costs of Health Care Administration in the United States and Canada, 1999 [13].
4. Conclusion
This study indicates that the universal healthcare system performs better than the healthcare system in the United States in both care delivery and coverage, as it provides easy access and comprehensive coverage. However, the multiple private payers in the United Healthcare system create strong competition that stimulates the growth of innovations. A new idea of the public innovation system comes up that might work well under the universal healthcare system. A publicly operated healthcare innovations system has three major benefits: (1) reducing the price of innovations, as the government is a non-profit driven organization; (2) returning the revenue to the government; (3) allocating resources efficiently by utilizing national funds, public institutions, and hospitals. Although the universal health system may week the incentive for innovation, there are many opportunities for it to enhance the ability to provide better treatment methods. It is impossible to list all of the healthcare-related issues impacting people's quality of life, but we examine the most important causes in this study.
References
[1]. Morgan, K. The Welfare State Nobody Knows: Debunking Myths about U.S. Social Policy and Welfare Discipline: Discourse, Governance, and Globalization. Perspectives on Politics, 6(1), 177-178 (2008). doi:10.1017/S1537592708080274
[2]. Vladeck B. Universal health insurance in the United States: reflections on the past, the present, and the future. Am J Public Health. Jan;93(1):16-9 (2003). doi: 10.2105/ajph.93.1.16. PMID: 12511377; PMCID: PMC1447684.
[3]. Eric C. Schneider et al., (2021) Mirror, Mirror 2021 — Reflecting Poorly: Health Care in the U.S. Compared to Other High-Income Countries, Commonwealth Fund, Aug. https://doi.org/10.26099/01DV-H208
[4]. Vita MG, Sacher S. The Competitive Effects of Not-For-Profit Hospital Mergers: a Case Study. Journal of Industrial Economics, vol. 49, no. 1 (2001).
[5]. Lipsitz LA. Understanding health care as a complex system: the foundation for unintended consequences. JAMA. Jul 18;308(3):243-4 (2012). doi: 10.1001/jama.2012.7551. PMID: 22797640; PMCID: PMC3511782.
[6]. Largest health insurance companies of 2023. value penguin. (n.d.). https://www.valuepenguin.com/largest-health-insurance-companies
[7]. Andreja Detiček, Igor Locatelli, Mitja Kos, Patient Access to Medicines for Rare Diseases in European Countries, Value in Health, Volume 21, Issue 5, pp.553-560 (2018), https://doi.org/10.1016/j.jval.2018.01.007.
[8]. James D. Chambers, PhD, Ari D. Panzer, BS, David D. Kim, PhD, Nikoletta M. Margaretos, BA, Peter J. Neumann, ScD, Variation in US Private Health Plans’ Coverage of Orphan Drugs, The American Journal of Managed Care, October, Volume 25, Issue 10 (2019). https://www.ajmc.com/view/variation-in-us-private-health-plans-coverage-of-orphan-drugs
[9]. Gammie, T., Lu, C. Y., & Ud-Din Babar, Z. Access to Orphan Drugs: A Comprehensive Review of Legislations, Regulations and Policies in 35 Countries. PLoS ONE, 10(10) (2014). https://doi.org/10.1371/journal.pone.0140002
[10]. Bloom DE, Khoury A, Subbaraman R. The promise and peril of universal health care. Science. 2018 Aug 24;361(6404):eaat9644. doi: 10.1126/science.aat9644. PMID: 30139847; PMCID: PMC6510304.
[11]. Industry market research, reports, and Statistics. IBISWorld. (n.d.). https://www.ibisworld.com/industry-statistics/employment/health-medical-insurance-united-states/#:~:text=There%20are%20563%2C366%20people%20employed,the%20US%20as%20of%202023.
[12]. Health Insurance Ceo Salary | comparably. https://www.comparably.com/salaries/salaries-for-ceo
[13]. Woolhandler, S., Campbell, T. M., & Himmelstein, D. U. (n.d.). Costs of Health Care Administration in the United States and Canada. The new England journal of medicine. https://www.nejm.org/doi/full/10.1056/NEJMsa022033
Cite this article
Sun,B. (2023). Comparison between the private healthcare system and the universal healthcare system in the U.S.. Theoretical and Natural Science,8,46-52.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Modern Medicine and Global Health
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. Morgan, K. The Welfare State Nobody Knows: Debunking Myths about U.S. Social Policy and Welfare Discipline: Discourse, Governance, and Globalization. Perspectives on Politics, 6(1), 177-178 (2008). doi:10.1017/S1537592708080274
[2]. Vladeck B. Universal health insurance in the United States: reflections on the past, the present, and the future. Am J Public Health. Jan;93(1):16-9 (2003). doi: 10.2105/ajph.93.1.16. PMID: 12511377; PMCID: PMC1447684.
[3]. Eric C. Schneider et al., (2021) Mirror, Mirror 2021 — Reflecting Poorly: Health Care in the U.S. Compared to Other High-Income Countries, Commonwealth Fund, Aug. https://doi.org/10.26099/01DV-H208
[4]. Vita MG, Sacher S. The Competitive Effects of Not-For-Profit Hospital Mergers: a Case Study. Journal of Industrial Economics, vol. 49, no. 1 (2001).
[5]. Lipsitz LA. Understanding health care as a complex system: the foundation for unintended consequences. JAMA. Jul 18;308(3):243-4 (2012). doi: 10.1001/jama.2012.7551. PMID: 22797640; PMCID: PMC3511782.
[6]. Largest health insurance companies of 2023. value penguin. (n.d.). https://www.valuepenguin.com/largest-health-insurance-companies
[7]. Andreja Detiček, Igor Locatelli, Mitja Kos, Patient Access to Medicines for Rare Diseases in European Countries, Value in Health, Volume 21, Issue 5, pp.553-560 (2018), https://doi.org/10.1016/j.jval.2018.01.007.
[8]. James D. Chambers, PhD, Ari D. Panzer, BS, David D. Kim, PhD, Nikoletta M. Margaretos, BA, Peter J. Neumann, ScD, Variation in US Private Health Plans’ Coverage of Orphan Drugs, The American Journal of Managed Care, October, Volume 25, Issue 10 (2019). https://www.ajmc.com/view/variation-in-us-private-health-plans-coverage-of-orphan-drugs
[9]. Gammie, T., Lu, C. Y., & Ud-Din Babar, Z. Access to Orphan Drugs: A Comprehensive Review of Legislations, Regulations and Policies in 35 Countries. PLoS ONE, 10(10) (2014). https://doi.org/10.1371/journal.pone.0140002
[10]. Bloom DE, Khoury A, Subbaraman R. The promise and peril of universal health care. Science. 2018 Aug 24;361(6404):eaat9644. doi: 10.1126/science.aat9644. PMID: 30139847; PMCID: PMC6510304.
[11]. Industry market research, reports, and Statistics. IBISWorld. (n.d.). https://www.ibisworld.com/industry-statistics/employment/health-medical-insurance-united-states/#:~:text=There%20are%20563%2C366%20people%20employed,the%20US%20as%20of%202023.
[12]. Health Insurance Ceo Salary | comparably. https://www.comparably.com/salaries/salaries-for-ceo
[13]. Woolhandler, S., Campbell, T. M., & Himmelstein, D. U. (n.d.). Costs of Health Care Administration in the United States and Canada. The new England journal of medicine. https://www.nejm.org/doi/full/10.1056/NEJMsa022033