






1. Introduction
The intricate and multifaceted realms of human emotion and psychological well-being have been a source of enduring fascination for scholars and practitioners alike. In this vast and intricate landscape, depression and anxiety emerge as towering peaks, casting their long shadows across the lives of countless individuals. While these two distinct mental health conditions manifest differently, they share a common thread of profound and often debilitating psychological distress. Given their pervasive prevalence, depression and anxiety have become enduring subjects of concern, sparking extensive research, study, and exploration.
This academic research paper embarks on a profound journey into the intricacies of this complex terrain, driven by the objective of unraveling the multifaceted dimensions of depression and anxiety. Its aim is to provide a comprehensive synthesis of the current state of knowledge in the field, drawing upon a diverse and extensive body of literature. In the pages that follow, the author traverses a diverse landscape of research and scholarship to illuminate several key facets of these psychological and mental health issues.
Within this exploration, the author delves into the prevalence of depression and anxiety, shedding light on the scope of these conditions within society. They navigate the intricate web of risk factors contributing to their onset and progression, offering a deeper understanding of the complex interplay of variables. They scrutinize the profound impact that depression and anxiety exert on individuals, families, and communities, recognizing the far-reaching consequences of these conditions. Finally, they embark on a comprehensive exploration of the available interventions and treatments, exploring the multifarious strategies that aim to alleviate the burden of these disorders.
As the author ventures through this intricate terrain, they are confronted with the stark reality that depression and anxiety are not isolated experiences but rather intricate threads in the fabric of human existence. It is my hope that this research paper will contribute to a deeper and more nuanced comprehension of these mental health challenges, ultimately paving the way for more effective strategies of intervention and treatment. In doing so, they endeavor to illuminate the path toward improved psychological well-being for individuals and the broader society.
2. Literature review
2.1. Prevalence of Depression and Anxiety
The pervasive impact of depression and anxiety knows no bounds, transcending the confines of geography, culture, and demographics. These insidious mental health conditions afflict a staggering number of individuals worldwide, surpassing the threshold of 280 million people, with anxiety and depressive disorders reigning as the most prevalent [1]. This stark reality confronts us on a global scale, as the relentless surge of depression and anxiety disorders continues unabated. Adding to this grim picture, the author is reminded that more than 700,000 lives are tragically lost to suicide each year [1].
Within the United States, a comprehensive study has estimated that a staggering 16.6% of adults grapple with major depressive disorder during their lifetime, while an equally concerning 18.1% contend with the burden of anxiety disorders [2]. These staggering statistics underscore the gravity of our inquiry into these conditions and emphasize the urgency of comprehending their widespread prevalence.
The author aspires to shed light on the multifaceted dimensions of depression and anxiety and embarks on this journey of exploration and understanding, it is imperative to acknowledge the immense scope of these mental health challenges, recognizing their far-reaching impact on individuals, families, and communities worldwide. Through diligent examination and comprehensive research, ultimately contributes to more effective strategies for intervention, treatment, and support.
2.2. Risk Factors
As the author embarks on a profound exploration of depression and anxiety, she finds herself in the intricate realm of their etiology. The origins of these complex conditions are far from monolithic; rather, they are shaped by a dynamic interplay of genetic, environmental, and psychological factors. The journey toward comprehending the intricate pathways leading to depression and anxiety is of paramount significance. It is through this understanding that she gains the tools necessary for early detection, effective prevention, and the development of precisely targeted interventions [3].
In this intricate web of causation, genetic predispositions intertwine with environmental influences, forging a unique narrative for everyone affected by these conditions. Unraveling this complex tapestry requires a multifaceted approach, one that acknowledges the diverse range of factors at play. Through meticulous research and comprehensive analysis, she endeavors to illuminate the pathways that lead to these conditions, ultimately striving to offer hope, support, and relief to those who grapple with the burdens of depression and anxiety.
2.2.1. Family. History and Genetics. The intricate puzzle of depression's origins takes us deeper into the realm of genetics, where familial history emerges as a significant factor. It has been observed that a family history of depression can heighten the likelihood of an individual experiencing it [4]. The intricate dance between genetics and depression is further underscored by research suggesting that heritability for major depression may be as substantial as 40–50% [5].
To unveil the role of genetics in this complex narrative, researchers have turned to twin studies. These investigations are founded on the premise that identical twins, who share 100% of their genes, should exhibit a higher concordance rate for depression if genes play a significant role in its development. In contrast, fraternal twins, who share only 50% of their genes, should demonstrate a lower concordance rate. The findings from such studies offer compelling evidence of the genetic underpinnings of depression, as they reveal that identical twins indeed have a significantly higher chance of sharing the condition compared to non-identical twins [5].
2.2.2. Chronic Stress. The intricate relationship between chronic stress and its impact on mental health, particularly the development of depression, is a compelling area of study. Prolonged exposure to chronic stress can erode the body's once-healthy stress response, setting the stage for the emergence of depression in susceptible individuals. At the core of this phenomenon lies the overactivity of the brain's Hypothalamic-Pituitary-Adrenal (HPA) axis, a vital system responsible for regulating stress responses. This overactivity leads to the excessive release of epinephrine and cortisol, hormones that play pivotal roles in the body's response to stress [5].
Extensive research has shed light on the association between HPA axis dysfunction and depression, revealing that approximately 70% of individuals with depression exhibit abnormalities within this crucial system [5]. This finding underscores the intricate interplay between chronic stress, neurobiological processes, and the onset of depression.
2.2.3. History of Trauma. The intricate relationship between Major Depressive Disorder (MDD) and a history of traumatic experiences unveils a compelling dimension of this complex condition. A profound exploration into the lives of individuals with MDD reveals that they bear a significantly heavier burden of past trauma, encompassing sexual, physical, and emotional abuse, in comparison to those without MDD [5].
Startling statistics underscore this connection, as 62.5% of participants diagnosed with MDD reported experiencing more than two traumatic events in their lives. In stark contrast, only 28.4% of participants in the healthy control group acknowledged similar experiences [5]. This stark disparity underscores the profound impact of traumatic events on the development and manifestation of MDD.
2.2.4. Gender. Gender disparities in the prevalence of depression cast a spotlight on an essential aspect of this multifaceted condition. The statistics reveal a significant imbalance, with women more likely to grapple with depression compared to their male counterparts. As per the World Health Organization, the prevalence of depression stands at 4% among men and 6% among women [1].
This gender disparity extends beyond mere statistics, as women often report experiencing more stress and higher rates of trauma than men [5]. These heightened stress levels and increased exposure to traumatic events contribute to a complex web of factors that may predispose women to depression.
A striking statistic further emphasizes the gender-specific burden of depression, with approximately 1 in 8 women expected to experience depression in their lifetime [5]. This staggering figure underscores the pressing need for tailored interventions, support, and research focused on addressing the unique challenges women face in the context of mental health.
2.2.5. Poor Nutrition. The intricate relationship between nutrition and mental health unveils another layer of complexity in our understanding of depression. Research underscores the profound impact of diet on brain function, shedding light on the significance of making informed dietary choices for mental well-being [5].
Evidence suggests that a diet predominantly consisting of processed foods may elevate an individual's risk of experiencing depression. This finding highlights the critical role of dietary quality in safeguarding mental health. The consumption of processed foods, often laden with artificial additives, preservatives, and unhealthy fats, may disrupt the delicate balance of neurotransmitters in the brain, potentially contributing to depressive symptoms [5].
Furthermore, the link between dietary choices and depression extends to the type of carbohydrates consumed. Research indicates that an excessive intake of simple carbohydrates is associated with an increased likelihood of experiencing depressive symptoms, particularly among women [5]. This association underscores the importance of balanced, nutrient-rich diets in supporting mental well-being.
2.2.6. Unresolved Grief or Loss. The intricate connection between grief, loss, and depression introduces a profound layer of understanding into the realm of mental health. While sadness and grief are natural responses to significant life events, they can sometimes trigger more severe symptoms of depression, such as thoughts of suicide or feelings of worthlessness [4]. This intersection between grief and depression underscores the importance of recognizing when normal emotional responses may escalate into more complex mental health challenges.
Statistics reveal that approximately 1 in 10 bereaved adults experiences prolonged grief [5]. This protracted mourning process, characterized by enduring emotional pain and distress, can pave the way for grief-related major depression. This phenomenon sheds light on the enduring impact of loss and the potential for grief to evolve into a debilitating mental health condition.
2.2.7. Personality Traits. The correlation between depression and the "Big Five" personality traits adds another layer of complexity to our understanding of mental health. The study's findings [5] indicate that individuals with depression may exhibit specific personality characteristics and tendencies, shedding light on the diverse manifestations of this condition. These personality traits can help us identify potential indicators of depression and tailor interventions accordingly.
2.2.8. Medication and Substance Use. The association between certain medications and substance-induced depression adds another layer of complexity to the understanding of depression. Medications can have a significant impact on an individual's mood and mental well-being, and it's essential to recognize the role of these substances in contributing to depressive symptoms [5].
2.3. Impact on Individuals
The far-reaching consequences of anxiety and depressive disorders underscore the urgency of addressing these conditions comprehensively. The impact of these disorders extends well beyond the individual level, affecting various aspects of society, including work environments, family dynamics, and overall community well-being [6-8].
2.4. Intervention and Treatment
The availability of effective interventions and treatments is pivotal in addressing the challenges posed by depression and anxiety. Recognizing the diverse nature of these conditions, various approaches have been developed to cater to individuals' unique needs and circumstances [9][10].
3. Methodology
The author utilized three machine learning models: the logistic regression model, the KNN model, and the CART model to conduct research on the causes of depression.
First, the random number seed was set to 202307, and the data set of 1503 samples was randomly divided into a training set (1202 samples) and a testing set (301 samples) following a 4:1 ratio. Next, the collected data were coded, assigning “No” to 0 and “Yes” to 1 in the Depressed variable. Additionally, the author utilized the “caret::train Control()” function to define specific parameters for the “caret::train()” function. The method parameter was set to “cv,” and the number parameter was set to 5. Subsequently, the processed data were used sequentially for model construction.
3.1. Logistic Regression Model
Logistic regression is a linear classification algorithm that maps the output of a linear regression to a probability space using a log-odds function. Logistic Regression is a commonly utilized classification algorithm, particularly for binary classification problems. The fundamental concept of logistic regression is to transform the output of linear regression into the probability space using the logistic function, achieving classification.
Initially, she employed the "caret::train()" function to establish a range of tuning parameters for various classification and regression techniques. Each model was fitted, and a performance measure based on resampling was computed. During this process, the method parameter was configured as "glm," and the training dataset was used as the input data.
Next, she utilized the “predict()” function to evaluate and predict the model's performance on the test set. This involved computing the model's confusion matrix and setting the parameter mode to compute derived metrics based on the confusion matrix. The type parameter was set to “prob,” and the testing dataset was used as the input data.
Subsequently, she employed the "caret::confusionMatrix()" function to compute a cross-tabulation comparing the observed and predicted classes, along with relevant statistics. Additionally, she calculated the FPR score, FNR score, ACC score, Precision score, Recall score, and F-score. She used the “pROC::roc()” function and the “pROC::plot.roc()” function to plot an ROC curve.
3.2. KNN Model
The K-Nearest Neighbor (KNN) algorithm stands out as one of the fundamental and straightforward machine learning algorithms applicable to both classification and regression tasks. KNN's classification process revolves around assessing the dissimilarity between distinct feature values. In essence, the KNN algorithm operates on a straightforward principle: for any input vector in an n-dimensional space, representing a specific point within the feature realm, the output corresponds to the category label or predicted value tied to that particular feature vector. KNN distinguishes itself from other machine learning algorithms in that it doesn't undergo a conventional learning phase. Instead, it relies on training data to segment the feature vector space, utilizing the outcome of this segmentation as the ultimate algorithmic model.
Initially, she employed the "caret::train()" function to establish a grid of tuning parameters, which encompassed various classification and regression techniques. Subsequently, she applied these parameters to fit each model and compute a performance measure based on resampling. In this case, the method parameter was configured as "knn," the tuneLength parameter was specified as 20, and the training dataset served as the input data. The optimal lambda value, denoted as "k," was determined to be 5.
Next, she used the “predict()” function to reason about and predict the model's performance on the test set, compute the model's confusion matrix, and set the parameter mode to compute the derived metrics based on the confusion matrix. The type parameter was set to “prob” and the testing dataset was as the input data.
Then, she employed the "caret::confusionMatrix()" function to compute a cross-tabulation that juxtaposed the observed and predicted classes. This analysis was accompanied by the calculation of pertinent statistics.
In addition, she calculated the FPR score, FNR score, ACC score, Precision score, Recall score, and F-score. And she used “pROC::roc()” function and “pROC::plot.roc()” function to plot a ROC curve.
3.3. CART Model
The CART algorithm, an abbreviation for Classification and Regression Tree Algorithm, is a variant of decision tree algorithms, alongside ID3 and C4.5. It functions through dichotomous recursive partitioning, splitting the current sample into two sub-samples. This results in a binary tree structure where each non-leaf node generates two branches, allowing for "yes" or "no" outcomes in decision-making. Even when a feature possesses multiple values, CART's binary nature means it consistently divides data into two subsets. The algorithm unfolds in two main stages: firstly, recursively dividing samples during the tree-building process, and secondly, employing pruning techniques using validation data.
First, the author used “randomForest::randomForest()” function to implement Breiman's random forest algorithm (based on Breiman and Cutler's original Fortran code) for classification and regression. The ntree parameter was set to 500, the mtry parameter was set to 3, and the training dataset was as the input data.
Next, she used the “predict()” function to reason about and predict the model's performance on the test set, compute the model's confusion matrix, and set the parameter mode to compute the derived metrics based on the confusion matrix. The testing dataset was as the input data.
Following that, she utilized the "caret::confusionMatrix()" function to generate a cross-tabulation involving the observed and predicted classes, while also deriving relevant statistics from this analysis.
In addition, she calculated the FPR score, FNR score, ACC score, Precision score, Recall score, and F-score. And she used “pROC::roc()” function and “pROC::plot.roc()” function to plot a ROC curve.
3.4. Data Description
Each column of the data the author used is a variable and each row is a sample. In total, there are 1503 samples and 11 variables. The variables are "Timestamp", "Age", "Feeling sad", "Irritable towards people", "Trouble sleeping at night", "Problems concentrating or making decision", "loss of appetite", "Feeling of guilt", "Problems of bonding with people", "Suicide attempt", "Depressed".
"Timestamp" is the time when the respondent fills out the questionnaire.
"Age": 25-30 years old (181), 30-35 years old (338), 35-40 years old (349), 40-45 years old (364), 45-50 years old (271).
"Feeling sad": No (524), Sometimes (443), Yes (536)
"Irritable towards people": No (499), Sometimes (443), Yes (555)
"Trouble sleeping at night": No (418), Two or more days a week (640), Yes (445)
"Problems concentrating or making decision": No (583), Often (473), Yes (435)
"loss of appetite": No (841), Not at all (319), Yes (343)
"Feeling of guilt": No (624), Maybe (528), Yes (342)
"Problems of bonding with people": No (557), Sometimes (542), Yes (404)
"Suicide attempt": No (709), Not interested to say (335), Yes (459)
"Depressed": No (523), Yes (980)
4. Result
In a classification task, the model often outputs predicted probabilities or scores for each category. Typically, a threshold is set to classify instances into specific categories based on these scores. However, using metrics like precision, recall, and F1 score can be influenced by the choice of this threshold. The Receiver Operating Characteristic (ROC) curve addresses this issue by evaluating model performance across various thresholds, making it a valuable tool for assessing classification models.
The False Positive Rate (FPR) is plotted against the True Positive Rate (TPR) on the horizontal axis of the ROC curve. A perfect model would have its ROC curve in the upper-left corner, where FPR is 0, TPR is 1, and all samples are correctly classified with no false positives or false negatives.
Creating an ROC curve is a straightforward process. First, sort the samples by their predicted probabilities or scores. Then, for each threshold (predicted probability), calculate the corresponding FPR and TPR. Finally, connect these points to form the ROC curve. The curve's shape and how close it is to the upper-left corner indicate the model's performance, with a curve closer to that corner representing better model accuracy and effectiveness.
The region below the ROC curve is known as the AUC (region Under Curve). The area below the ROC curve and the AUC are both indicators of how good a model is.
4.1. Logistic Regression Model
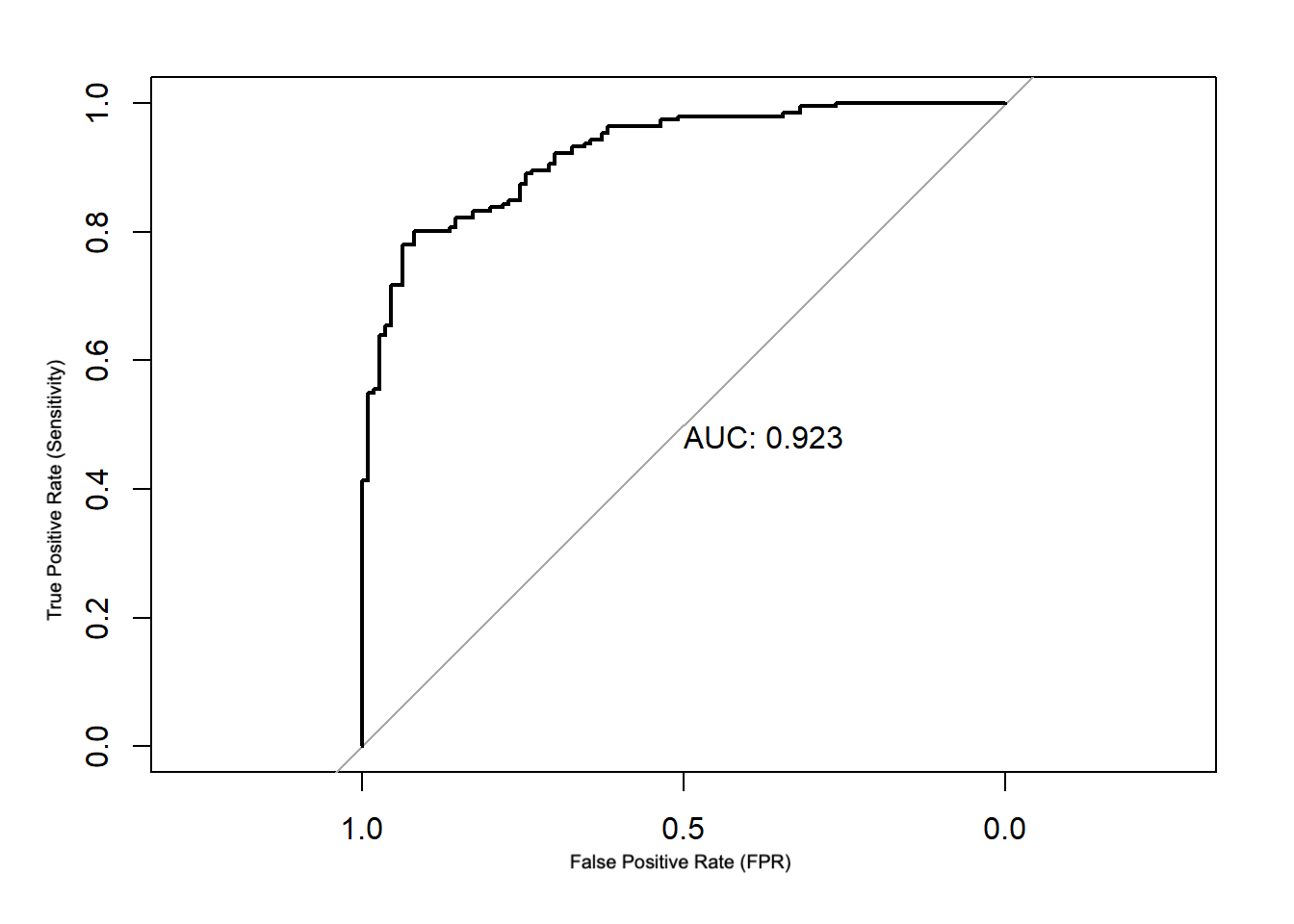
Figure 1. ROC Curve for Logistic Regression Model.
Figure 1 displays the ROC curve for the logistic regression model. The findings show the following performance metrics: an F-score of 0.762, an Accuracy (ACC) of 0.841, a Precision of 0.837, a Recall of 0.700, a False Positive Rate (FPR) of 0.0785, and an Area Under the Curve (AUC) of 0.923.
These metrics collectively indicate that the logistic regression model is proficient at classification tasks, achieving a high level of accuracy and precision. Additionally, the AUC value of 0.923 suggests that the model's performance is excellent, further confirming its ability to discriminate between classes effectively.
4.2. KNN Model
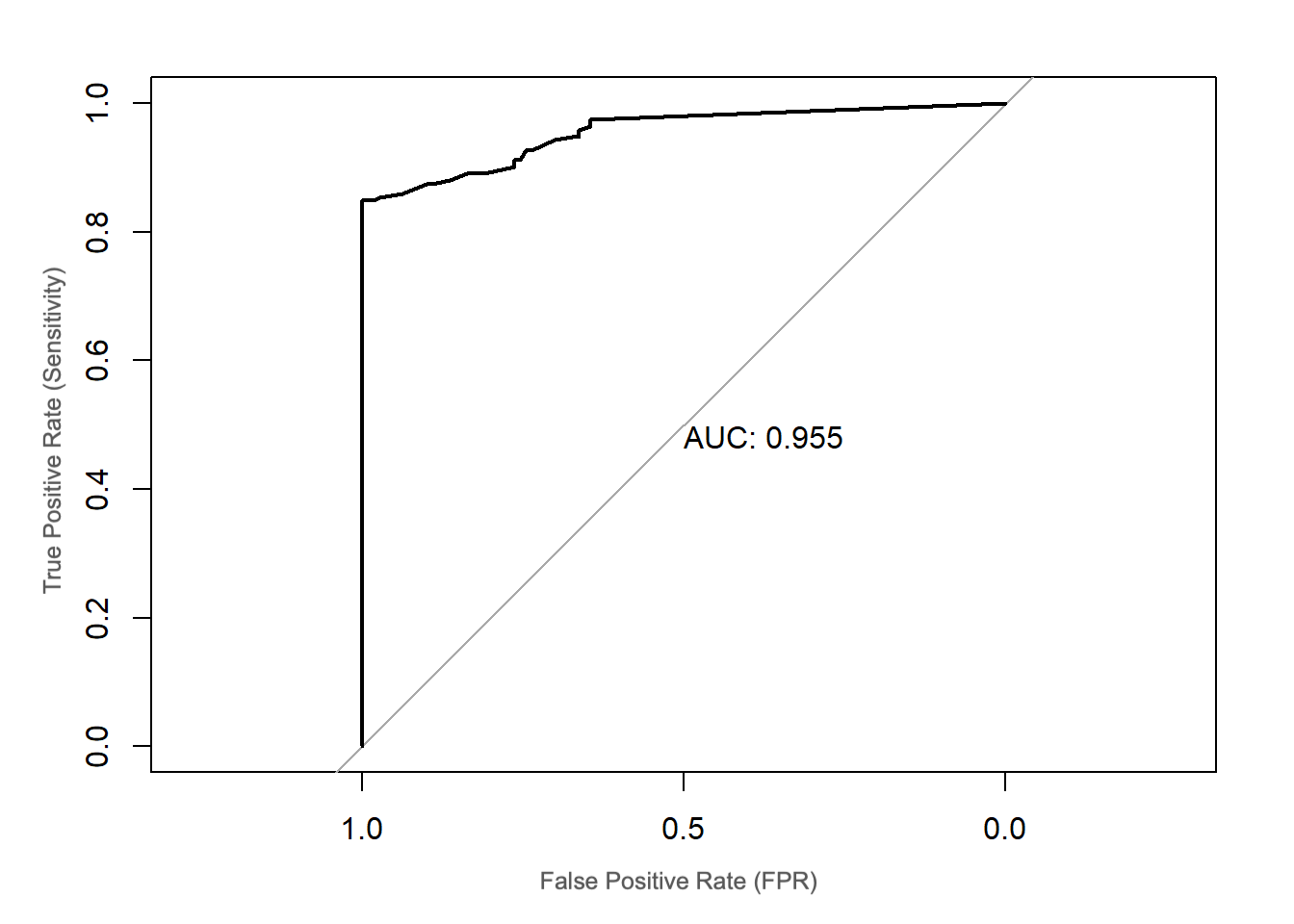
Figure 2. ROC Curve for KNN Model.
Figure 2 displays the ROC curve for the KNN model. The outcomes show the following performance metrics: an FPR of 0.0838, a FNR of 0.255, an ACC of 0.854, a Precision of 0.837, a Recall of 0.745, an F-score of 0.788, and an AUC of 0.955.
These metrics highlight the KNN model's strong ability to perform classification tasks effectively. It achieves high accuracy, precision, and recall, indicating its proficiency in distinguishing between classes. Additionally, the remarkable AUC value of 0.955 further underscores the model's excellent performance in class separation.
4.3. CART Model
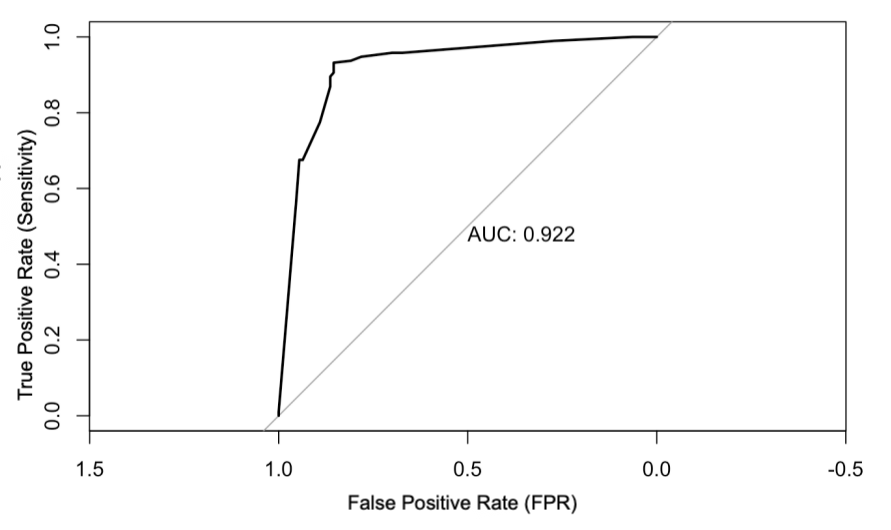
Figure 3. ROC Curve for CART Model.
Figure 3 displays the ROC curve for the CART model. The findings show the following performance metrics: 0.0681 for the False Positive Rate (FPR), 0.145 for the False Negative Rate (FNR), 0.904 for the Accuracy (ACC), 0.879 for the Precision, 0.855 for the Recall, 0.866 for the F-score, and 0.922 for the Area Under the Curve (AUC).
These metrics collectively emphasize the CART model's strong capability in performing classification tasks effectively. It achieves high accuracy, precision, and recall, signifying its proficiency in distinguishing between classes. Moreover, the notable AUC value of 0.922 further underscores the model's excellent performance in class separation.
Taking a broader perspective, when the author compares the AUC values of the three models, she finds that the KNN model boasts the highest AUC value at 0.955, suggesting that it exhibits superior classification capabilities. However, it's essential to note that the ROC curves for all three models appear somewhat jagged or not perfectly smooth. This observation could indicate the presence of overfitting during the model training process. Overfitting occurs when a model becomes excessively complex and fits the training data too closely, potentially leading to reduced generalizability on unseen data. Therefore, despite the high AUC values, there is a need to address the potential overfitting issue in these models.
5. Future outlooks
The findings offer valuable insights into addressing the challenges posed by depression. Firstly, it is imperative to enhance public education efforts aimed at raising awareness about depression's preventable and treatable nature. By eliminating the stigma associated with the condition and fostering a better understanding of depression within society, more individuals may be encouraged to seek treatment willingly. Simultaneously, there is a pressing need to bolster the medical system. This involves elevating the diagnostic and treatment standards in hospitals, increasing the training of mental health professionals, and expediting the development of innovative treatment approaches at the enterprise level. A dual-pronged approach, combining public education and healthcare system enhancement, is essential for significant progress in China's mental health initiatives.
Depression is not a mere act or pretense but rather a complex mood disorder rooted in the brain. It is intrinsically linked to genetic factors and results from the interplay between genes and the environment. The rehabilitation and treatment of individuals grappling with depression necessitate collaborative efforts between the government and the private sector.
Civil institutions and patient organizations provide crucial platforms for patients to connect, collaborate, and share their experiences. Through social welfare initiatives, the goal of patients helping each other and themselves can be achieved. Hospitals play a pivotal role by offering professional disease diagnosis, technical treatment services, and expert guidance for patients' rehabilitation journeys. Rehabilitation institutions can organize patients to engage in social work, impart essential rehabilitation skills, standardize depression treatment practices, and create favorable conditions for patients' recovery.
Through a multifaceted collaboration involving various stakeholders, each contributing their unique strengths, a comprehensive support network can be established. This collaborative effort ensures that all departments and organizations play their part, providing practical assistance to patients and contributing to meaningful progress in the battle against depression.
6. Conclusion
Following the comprehensive analysis presented above, it becomes evident that depression is intricately linked to a range of observable phenomena. These include but are not limited to a persistent sense of sadness, sleep disturbances, contemplation of death or suicide, irritability, appetite disturbances, reduced concentration, and interpersonal difficulties.
In summary, depression and anxiety represent substantial mental health issues that permeate various aspects of individuals' lives. This literature review has furnished an expansive understanding of their prevalence, the intricate web of risk factors, the profound impact they exert, and the array of interventions available. By acknowledging the multifaceted nature of the factors influencing depression and anxiety, she underscores the necessity of formulating holistic strategies for their prevention and treatment. These conditions demand our continued attention and concerted efforts from various stakeholders to alleviate their burdens on individuals, families, and society at large.
References
[1]. World Health Organization. (2023, March 31). Depressive Disorder (Depression). World Health Organisation. https://www.who.int/news-room/fact-sheets/detail/depression
[2]. Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
[3]. Kalin, N. H. (2020). The Critical Relationship Between Anxiety and Depression. American Journal of Psychiatry, 177(5), 365–367. https://doi.org/10.1176/appi.ajp.2020.20030305
[4]. Bruce, D. F., & PhD. (2021, October 31). Are You at Risk for Depression? WebMD. https://www.webmd.com/depression/depression-are-you-at-risk
[5]. Pederson, T., & Arthur, S. (2021, June 2). Risk Factors for Depression: Genetics, Trauma, and More. Psych Central. https://psychcentral.com/depression/what-are-the-risk-factors-for-depression
[6]. Brenes, G. A. (2007). Anxiety, Depression, and Quality of Life in Primary Care Patients. Primary Care Companion to the Journal of Clinical Psychiatry, 9(6), 437–443. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2139931/
[7]. Negele, A., Kaufhold, J., Kallenbach, L., & Leuzinger-Bohleber, M. (2015). Childhood Trauma and Its Relation to Chronic Depression in Adulthood. Depression Research and Treatment, 2015(1), 1–11. https://doi.org/10.1155/2015/650804
[8]. Smalbrugge, M., Pot, A. M., Jongenelis, L., Gundy, C. M., Beekman, A. T. F., & Eefsting, J. A. (2006). The impact of depression and anxiety on well being, disability and use of health care services in nursing home patients. International Journal of Geriatric Psychiatry, 21(4), 325–332. https://doi.org/10.1002/gps.1466
[9]. Tiller, J. W. G. (2013). Depression and anxiety. Medical Journal of Australia, 199(6). https://www.mja.com.au/journal/2013/199/6/depression-and-anxiety#0_i1140732
[10]. Priya, A., Garg, S., & Tigga, N. P. (2020). Predicting Anxiety, Depression and Stress in Modern Life using Machine Learning Algorithms. Procedia Computer Science, 167(6), 1258–1267. https://doi.org/10.1016/j.procs.2020.03.442
Cite this article
Tang,J. (2023). The association between depression and anxiety. Theoretical and Natural Science,15,282-291.
Data availability
The datasets used and/or analyzed during the current study will be available from the authors upon reasonable request.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of EWA Publishing and/or the editor(s). EWA Publishing and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
About volume
Volume title: Proceedings of the 2nd International Conference on Modern Medicine and Global Health
© 2024 by the author(s). Licensee EWA Publishing, Oxford, UK. This article is an open access article distributed under the terms and
conditions of the Creative Commons Attribution (CC BY) license. Authors who
publish this series agree to the following terms:
1. Authors retain copyright and grant the series right of first publication with the work simultaneously licensed under a Creative Commons
Attribution License that allows others to share the work with an acknowledgment of the work's authorship and initial publication in this
series.
2. Authors are able to enter into separate, additional contractual arrangements for the non-exclusive distribution of the series's published
version of the work (e.g., post it to an institutional repository or publish it in a book), with an acknowledgment of its initial
publication in this series.
3. Authors are permitted and encouraged to post their work online (e.g., in institutional repositories or on their website) prior to and
during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work (See
Open access policy for details).
References
[1]. World Health Organization. (2023, March 31). Depressive Disorder (Depression). World Health Organisation. https://www.who.int/news-room/fact-sheets/detail/depression
[2]. Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
[3]. Kalin, N. H. (2020). The Critical Relationship Between Anxiety and Depression. American Journal of Psychiatry, 177(5), 365–367. https://doi.org/10.1176/appi.ajp.2020.20030305
[4]. Bruce, D. F., & PhD. (2021, October 31). Are You at Risk for Depression? WebMD. https://www.webmd.com/depression/depression-are-you-at-risk
[5]. Pederson, T., & Arthur, S. (2021, June 2). Risk Factors for Depression: Genetics, Trauma, and More. Psych Central. https://psychcentral.com/depression/what-are-the-risk-factors-for-depression
[6]. Brenes, G. A. (2007). Anxiety, Depression, and Quality of Life in Primary Care Patients. Primary Care Companion to the Journal of Clinical Psychiatry, 9(6), 437–443. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2139931/
[7]. Negele, A., Kaufhold, J., Kallenbach, L., & Leuzinger-Bohleber, M. (2015). Childhood Trauma and Its Relation to Chronic Depression in Adulthood. Depression Research and Treatment, 2015(1), 1–11. https://doi.org/10.1155/2015/650804
[8]. Smalbrugge, M., Pot, A. M., Jongenelis, L., Gundy, C. M., Beekman, A. T. F., & Eefsting, J. A. (2006). The impact of depression and anxiety on well being, disability and use of health care services in nursing home patients. International Journal of Geriatric Psychiatry, 21(4), 325–332. https://doi.org/10.1002/gps.1466
[9]. Tiller, J. W. G. (2013). Depression and anxiety. Medical Journal of Australia, 199(6). https://www.mja.com.au/journal/2013/199/6/depression-and-anxiety#0_i1140732
[10]. Priya, A., Garg, S., & Tigga, N. P. (2020). Predicting Anxiety, Depression and Stress in Modern Life using Machine Learning Algorithms. Procedia Computer Science, 167(6), 1258–1267. https://doi.org/10.1016/j.procs.2020.03.442